Kambugu Andrew, Meya David B, Rhein Joshua, O'Brien Meagan, Janoff Edward N, Ronald Allan R, Kamya Moses R, Mayanja-Kizza Harriet, Sande Merle A, Bohjanen Paul R, Boulware David R
Infectious Disease Institute, Makerere University, Kampala Uganda.
Clin Infect Dis. 2008 Jun 1;46(11):1694-701. doi: 10.1086/587667.
Cryptococcal meningitis (CM) is the proximate cause of death in 20%-30% of persons with acquired immunodeficiency syndrome in Africa.
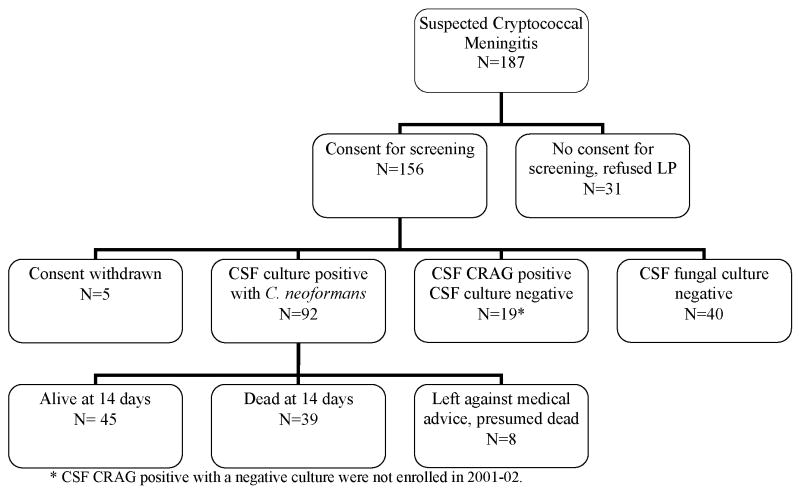
Two prospective, observational cohorts enrolled human immunodeficiency virus (HIV)-infected, antiretroviral-naive persons with CM in Kampala, Uganda. The first cohort was enrolled in 2001-2002 (n = 92), prior to the availability of highly active antiretroviral therapy (HAART), and the second was enrolled in 2006-2007 (n = 44), when HAART was available.
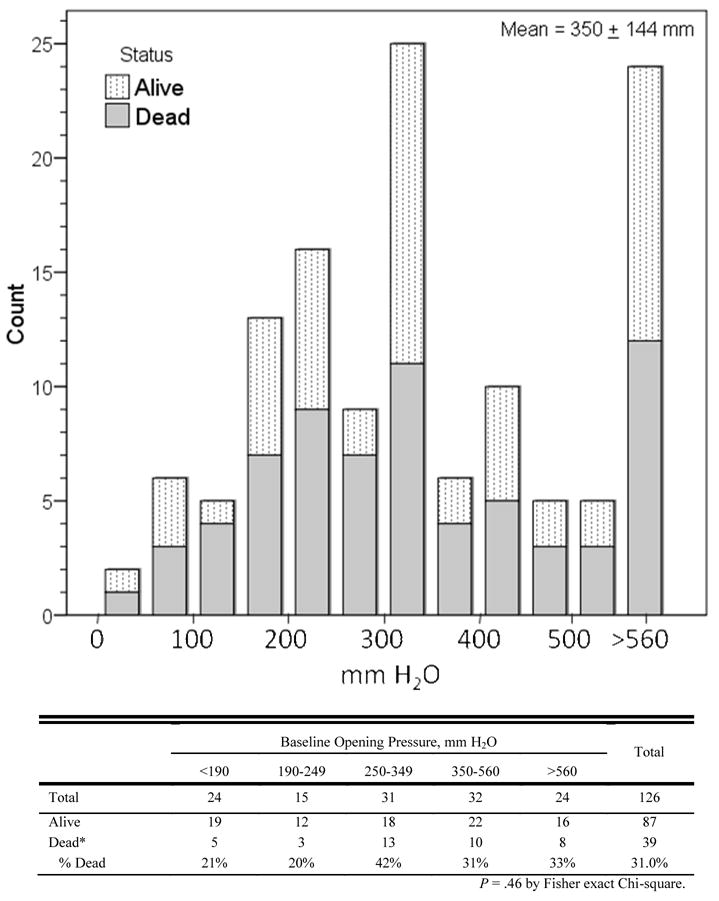
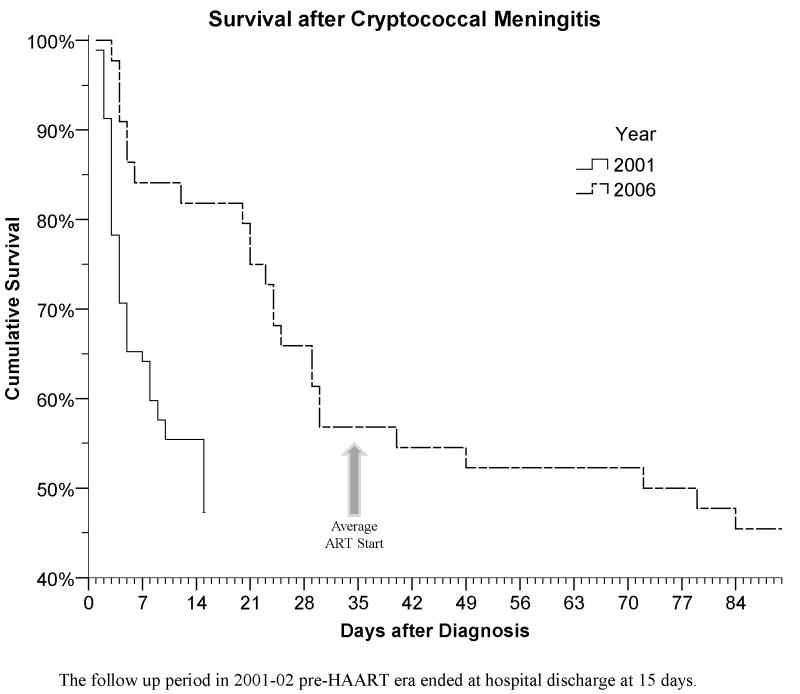
Ugandans presented with prolonged CM symptoms (median duration, 14 days; interquartile range, 7-21 days). The 14-day survival rates were 49% in 2001-2002 and 80% in 2006 (P < .001). HAART was started 35 +/- 13 days after CM diagnosis and does not explain the improved 14-day survival rate in 2006. In 2006-2007, the survival rate continued to decrease after hospitalization, with only 55% surviving to initiate HAART as an outpatient. Probable cryptococcal-related immune reconstitution inflammatory syndrome occurred in 42% of patients, with 4 deaths. At 6 months after CM diagnosis, 18 persons (41%) were alive and receiving HAART in 2007. The median cerebral spinal fluid (CSF) opening pressure was 330 mm H(2)O; 81% of patients had elevated pressure (>200 mm H(2)O). Only 5 patients consented to therapeutic lumbar puncture. There was a trend for higher mortality for pressures >250 mm H(2)O (odds ratio [OR], 2.1; 95% confidence interval [CI], 0.9-5.2; P = .09). Initial CSF WBC counts of <5 cells/mL were associated with failure of CSF sterilization (OR, 17.3; 95% CI, 3.1-94.3; P < .001), and protein levels <35 mg/dL were associated with higher mortality (OR, 2.0; 95% CI, 1.2-3.3; P = .007).
Significant CM-associated mortality persists, despite the administration of amphotericin B and HIV therapy, because of the high mortality rate before receipt of HAART and because of immune reconstitution inflammatory syndrome-related complications after HAART initiation. Approaches to increase acceptance of therapeutic lumbar punctures are needed.
在非洲,隐球菌性脑膜炎(CM)是20% - 30%获得性免疫缺陷综合征患者的直接死因。
两项前瞻性观察性队列研究纳入了乌干达坎帕拉感染人类免疫缺陷病毒(HIV)且未接受抗逆转录病毒治疗的CM患者。第一个队列于2001 - 2002年纳入(n = 92),当时高效抗逆转录病毒治疗(HAART)尚未普及;第二个队列于2006 - 2007年纳入(n = 44),此时HAART已可获得。
乌干达患者出现CM症状的时间较长(中位持续时间为14天;四分位间距为7 - 21天)。2001 - 2002年的14天生存率为49%,2006年为80%(P < 0.001)。HAART在CM诊断后35 ± 13天开始,这并不能解释2006年14天生存率的提高。在2006 - 2007年,住院后生存率持续下降,只有55%的患者存活至门诊开始接受HAART。42%的患者发生了可能与隐球菌相关的免疫重建炎症综合征,有4例死亡。在CM诊断后6个月,2007年有18人(41%)存活并接受HAART。脑脊液(CSF)初压中位数为330 mm H₂O;81%的患者压力升高(>200 mm H₂O)。只有5例患者同意进行治疗性腰椎穿刺。压力>250 mm H₂O的患者死亡率有升高趋势(比值比[OR]为2.1;95%置信区间[CI]为0.9 - 5.2;P = 0.09)。初始CSF白细胞计数<5个/毫升与CSF灭菌失败相关(OR为17.3;95% CI为3.1 - 94.3;P < 0.001),蛋白质水平<35 mg/dL与较高死亡率相关(OR为2.0;95% CI为1.2 - 3.3;P = 0.007)。
尽管使用了两性霉素B和HIV治疗,但由于在接受HAART之前死亡率高以及在开始HAART后出现与免疫重建炎症综合征相关的并发症,CM相关的显著死亡率仍然存在。需要采取措施提高对治疗性腰椎穿刺的接受度。