Portera Chia C, Walshe Janice M, Rosing Douglas R, Denduluri Neelima, Berman Arlene W, Vatas Ujala, Velarde Margarita, Chow Catherine K, Steinberg Seth M, Nguyen Diana, Yang Sherry X, Swain Sandra M
Medical Oncology Branch, National Cancer Institute, Bethesda, MD, USA.
Clin Cancer Res. 2008 May 1;14(9):2710-6. doi: 10.1158/1078-0432.CCR-07-4636.
To evaluate safety and efficacy of trastuzumab with pertuzumab in patients with human epidermal growth factor receptor 2 (HER2)-positive metastatic breast cancer who had progressive disease on trastuzumab-based therapy.
Patients with measurable HER2(+) metastatic breast cancer, < or = 3 trastuzumab-based regimens, and left ventricular ejection fraction (LVEF) > or = 55% received 8 or 6 mg/kg trastuzumab and 840 mg pertuzumab i.v. followed by 6 mg/kg trastuzumab and 420 mg pertuzumab every 3 weeks. Cardiac evaluation and tumor response were assessed every 3 and 6 weeks, respectively.
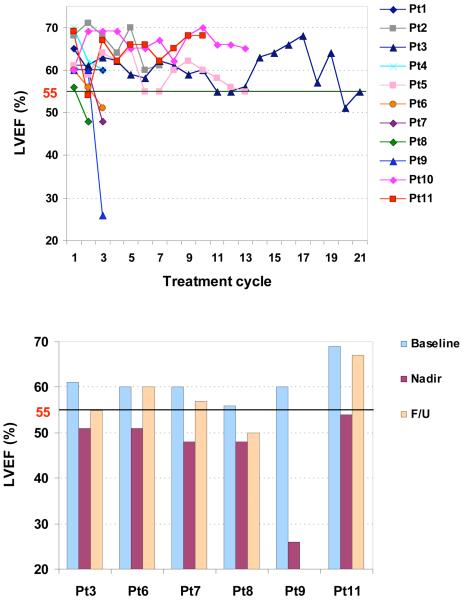
Eleven patients received 64 cycles of trastuzumab plus pertuzumab. A total of 92 echocardiograms and 8 cardiac magnetic resonance imaging studies were done. With the lower limit of normal LVEF 55%, left ventricular systolic dysfunction was observed in six patients, three grade 1, two grade 2, and one grade 3 according to the National Cancer Institute Common Terminology Criteria for Adverse Events. The objective response rate was 18%. Two patients had partial responses, three had stable disease, and six had progressive disease. The median time to progression was 6 weeks. In baseline tumors from formalin-fixed paraffin-embedded primary and/or metastatic tumor biopsies, pHER2-Y1248 trended toward an increase in patients with partial response compared with those with stable disease/progressive disease (P = 0.095).
Trastuzumab plus pertuzumab may have clinical benefit in selected patients who have previously been treated with trastuzumab. Cardiac toxicity, although asymptomatic in most cases, was associated with this treatment. Further evaluation of efficacy of this combination is required to define the overall risks and benefits.
评估曲妥珠单抗联合帕妥珠单抗用于接受过曲妥珠单抗治疗且病情进展的人表皮生长因子受体2(HER2)阳性转移性乳腺癌患者的安全性和疗效。
可测量的HER2(+)转移性乳腺癌患者,接受过≤3种基于曲妥珠单抗的治疗方案,且左心室射血分数(LVEF)≥55%,静脉注射8或6mg/kg曲妥珠单抗和840mg帕妥珠单抗,随后每3周静脉注射6mg/kg曲妥珠单抗和420mg帕妥珠单抗。分别每3周和6周评估心脏情况及肿瘤反应。
11例患者接受了64个周期的曲妥珠单抗加帕妥珠单抗治疗。共进行了92次超声心动图检查和8次心脏磁共振成像研究。以LVEF正常下限55%为标准,根据美国国立癌症研究所不良事件通用术语标准,6例患者出现左心室收缩功能障碍,其中3例为1级,2例为2级,1例为3级。客观缓解率为18%。2例患者部分缓解,3例病情稳定,6例病情进展。中位疾病进展时间为6周。在福尔马林固定石蜡包埋的原发性和/或转移性肿瘤活检的基线肿瘤中,与病情稳定/进展的患者相比,部分缓解患者的pHER2-Y1248有升高趋势(P = 0.095)。
曲妥珠单抗加帕妥珠单抗可能对先前接受过曲妥珠单抗治疗的特定患者有临床益处。心脏毒性虽然在大多数情况下无症状,但与这种治疗有关。需要进一步评估这种联合治疗的疗效,以确定总体风险和益处。