De Luca G, Gibson C M, Bellandi F, Murphy S, Maioli M, Noc M, Zeymer U, Dudek D, Arntz H-R, Zorman S, Gabriel H M, Emre A, Cutlip D, Biondi-Zoccai G, Rakowski T, Gyongyosi M, Marino P, Huber K, van't Hof A W J
Division of Cardiology, Maggiore della Carità Hospital, Eastern Piedmont University, Novara, Italy.
Heart. 2008 Dec;94(12):1548-58. doi: 10.1136/hrt.2008.141648. Epub 2008 May 12.
Even though time-to-treatment has been shown to be a determinant of mortality in primary angioplasty, the potential benefits from early pharmacological reperfusion by glycoprotein (Gp) IIb-IIIa inhibitors are still unclear. The aim of this meta-analysis was to combine individual data from all randomised trials conducted on facilitated primary angioplasty by the use of early Gp IIb-IIIa inhibitors.
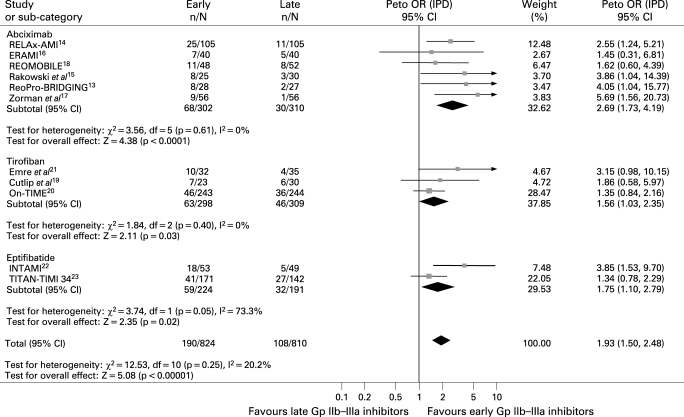
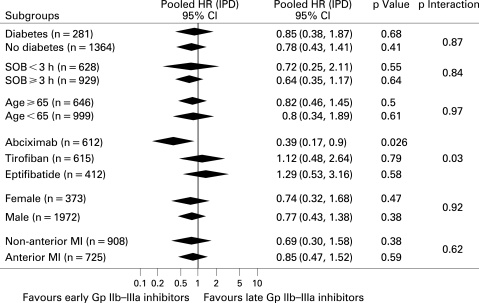
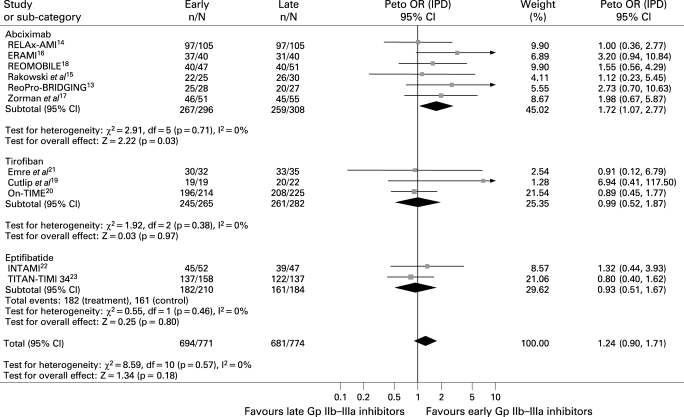
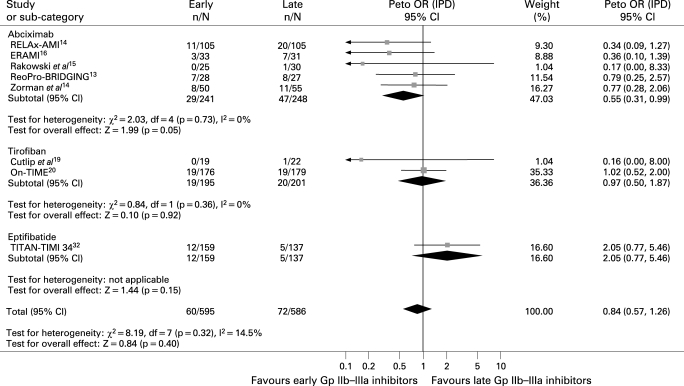
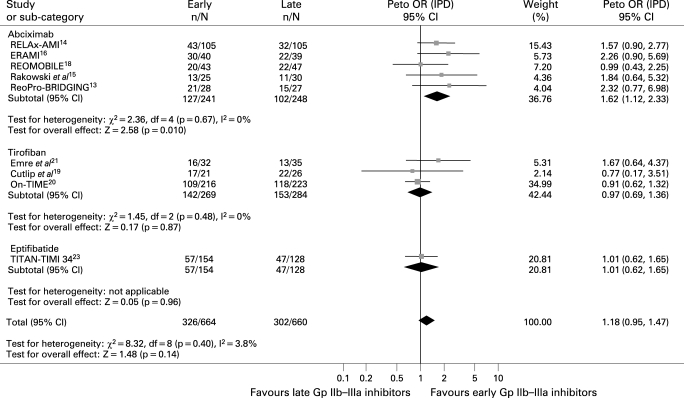
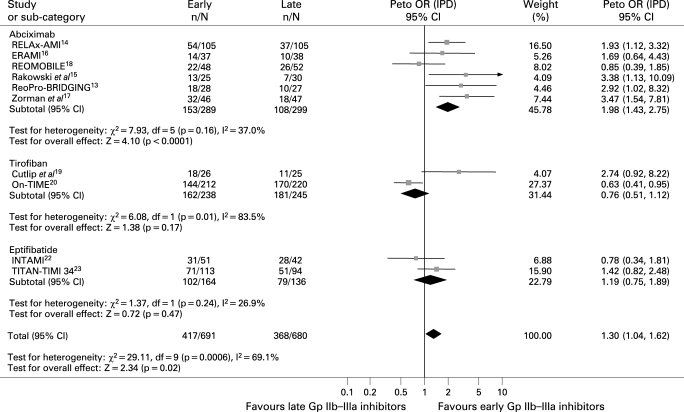
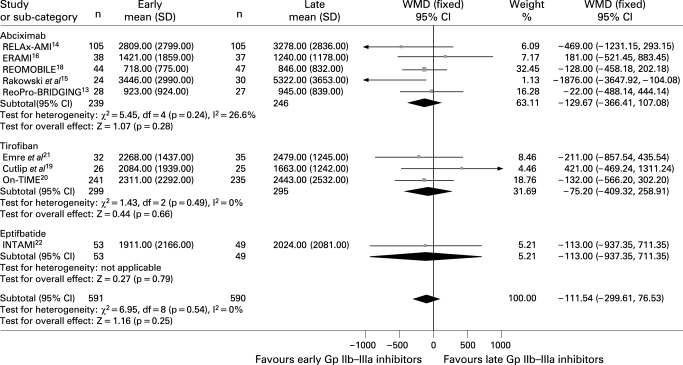
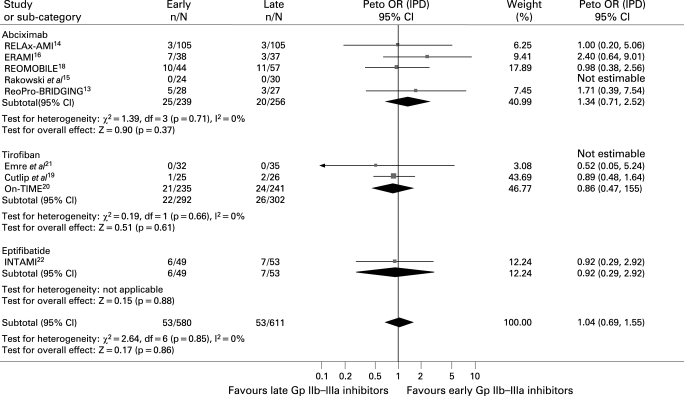
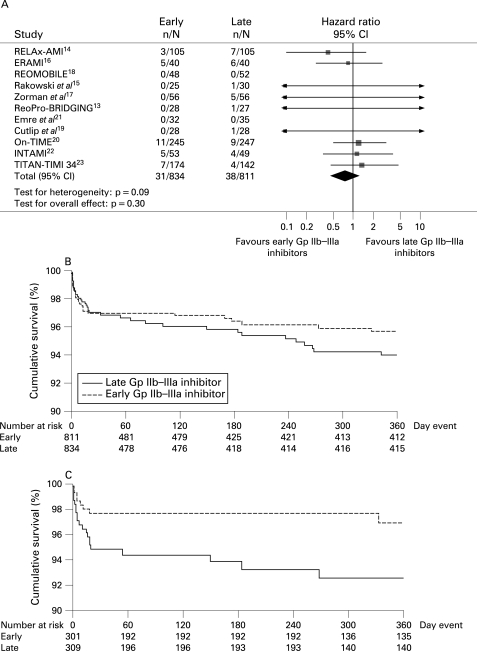
The literature was scanned by formal searches of electronic databases (MEDLINE, EMBASE) from January 1990 to October 2007. All randomised trials on facilitation by the early administration of Gp IIb-IIIa inhibitors in ST-segment elevation myocardial infarction (STEMI) were examined. No language restrictions were enforced. Individual patient data were obtained from 11 out of 13 trials, including 1662 patients (840 patients (50.5%) randomly assigned to early and 822 patients (49.5%) to late Gp IIb-IIIa inhibitor administration). Preprocedural Thrombolysis in Myocardial Infarction Study (TIMI) grade 3 flow was more frequent with early Gp IIb-IIIa inhibitors. Postprocedural TIMI 3 flow and myocardial blush grade 3 were higher with early Gp IIb-IIIa inhibitors but did not reach statistical significance except for abciximab, whereas the rate of complete ST-segment resolution was significantly higher with early Gp IIb-IIIa inhibitors. Mortality was not significantly different between groups, although early abciximab demonstrated improved survival compared with late administration, even after adjustment for clinical and angiographic confounding factors.
This meta-analysis shows that pharmacological facilitation with the early administration of Gp IIb-IIIa inhibitors in patients undergoing primary angioplasty for STEMI is associated with significant benefits in terms of preprocedural epicardial recanalisation and ST-segment resolution, which translated into non-significant mortality benefits except for abciximab.
尽管治疗时间已被证明是直接经皮冠状动脉腔内血管成形术(primary angioplasty)中死亡率的一个决定因素,但糖蛋白(Gp)IIb-IIIa抑制剂进行早期药物再灌注的潜在益处仍不明确。本荟萃分析的目的是合并所有关于使用早期Gp IIb-IIIa抑制剂进行易化直接经皮冠状动脉腔内血管成形术的随机试验的个体数据。
通过对1990年1月至2007年10月的电子数据库(MEDLINE、EMBASE)进行正式检索来筛选文献。检查了所有关于在ST段抬高型心肌梗死(STEMI)中早期给予Gp IIb-IIIa抑制剂进行易化治疗的随机试验。没有实施语言限制。从13项试验中的11项获得了个体患者数据,包括1662例患者(840例患者(50.5%)被随机分配接受早期Gp IIb-IIIa抑制剂治疗,822例患者(49.5%)接受晚期Gp IIb-IIIa抑制剂治疗)。早期使用Gp IIb-IIIa抑制剂时,术前心肌梗死溶栓试验(TIMI)3级血流更常见。早期使用Gp IIb-IIIa抑制剂时,术后TIMI 3级血流和心肌灌注分级3级更高,但除阿昔单抗外未达到统计学意义,而早期使用Gp IIb-IIIa抑制剂时完全ST段回落率显著更高。两组间死亡率无显著差异,尽管早期使用阿昔单抗与晚期给药相比显示出生存率提高,即使在对临床和血管造影混杂因素进行调整后也是如此。
本荟萃分析表明,在接受STEMI直接经皮冠状动脉腔内血管成形术的患者中,早期给予Gp IIb-IIIa抑制剂进行药物易化治疗在术前心外膜再通和ST段回落方面具有显著益处,除阿昔单抗外,这转化为不显著的死亡率益处。