Rathkopf Dana, Carducci Michael A, Morris Michael J, Slovin Susan F, Eisenberger Mario A, Pili Roberto, Denmeade Samuel R, Kelsen Moshe, Curley Tracy, Halter Melinda, Collins Connie, Fleisher Martin, Heller Glenn, Baker Sharyn D, Scher Howard I
Department of Medicine, Genitourinary Oncology Service, Memorial Sloan-Kettering Cancer Center, New York, NY 10021, USA.
J Clin Oncol. 2008 Jun 20;26(18):2959-65. doi: 10.1200/JCO.2007.15.1928.
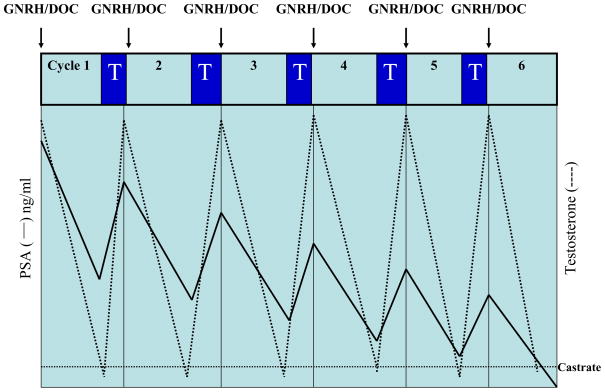
We evaluated rapid androgen cycling in combination with docetaxel for men with progressive noncastrate prostate cancers.
Noncastrate patients with <or= 6 months of hormone therapy were eligible. Cohort 1 (62 patients) received six 28-day cycles of docetaxel (75 mg/m(2)), leuprolide, and 7 days of topical testosterone. Cohort 2 (38 patients) received nine 21-day cycles of docetaxel (70 mg/m(2)), leuprolide, and 3 days of testosterone. The primary end point was the proportion of patients at 18 months who achieved noncastrate testosterone levels (> 150 ng/dL) and an undetectable prostate-specific antigen (PSA; <or= 0.05, <or= 0.5, or <or= 2.0 ng/mL with prior prostatectomy, radiation therapy, or no definitive therapy, respectively). Cytochrome P450 3A4 (CYP3A4) activity and docetaxel pharmacokinetics were evaluated.
A higher proportion of patients achieved the undetectable PSA outcome at 18 months in cohort 2 relative to cohort 1 (13% v 0%). The 16% incidence of febrile neutropenia was higher than that observed in patients was castration-resistant disease, which may have been related to a 50% reduction in overall docetaxel clearance in the noncastrate group. There was no alteration in CYP3A4 activity (P = .87) or docetaxel clearance (P = .88) between cycles.
The undetectable PSA end point allows for a rapid screening of interventions for further study. Increasing the number of docetaxel cycles after a shorter period of testosterone repletion, and a longer duration of testosterone depletion, increased the proportion of men who achieved an undetectable PSA. The higher-than-expected incidence of febrile neutropenia may have been related to the reduced overall docetaxel clearance in patients with noncastrate versus castrate testosterone levels.
我们评估了快速雄激素循环联合多西他赛用于进展期非去势前列腺癌男性患者的疗效。
激素治疗时间≤6个月的非去势患者符合条件。队列1(62例患者)接受六个28天周期的多西他赛(75mg/m²)、亮丙瑞林以及7天的外用睾酮治疗。队列2(38例患者)接受九个21天周期的多西他赛(70mg/m²)、亮丙瑞林以及3天的睾酮治疗。主要终点是18个月时达到非去势睾酮水平(>150ng/dL)且前列腺特异性抗原(PSA)检测不到(分别在既往接受前列腺切除术、放射治疗或未接受确定性治疗的情况下,PSA≤0.05、≤0.5或≤2.0ng/mL)的患者比例。评估了细胞色素P450 3A4(CYP3A4)活性和多西他赛的药代动力学。
与队列1相比,队列2中18个月时达到PSA检测不到这一结果的患者比例更高(13%对0%)。发热性中性粒细胞减少症的发生率为16%,高于去势抵抗性疾病患者中观察到的发生率,这可能与非去势组中多西他赛总体清除率降低50%有关。各周期之间CYP3A4活性(P = 0.87)或多西他赛清除率(P = 0.88)没有变化。
PSA检测不到这一终点可用于快速筛选干预措施以便进一步研究。在较短的睾酮补充期后增加多西他赛周期数,以及延长睾酮剥夺期,可提高达到PSA检测不到的男性患者比例。发热性中性粒细胞减少症的发生率高于预期,这可能与非去势睾酮水平患者中多西他赛总体清除率降低有关。