Karyana Muhammad, Burdarm Lenny, Yeung Shunmay, Kenangalem Enny, Wariker Noah, Maristela Rilia, Umana Ketut Gde, Vemuri Ram, Okoseray Maurits J, Penttinen Pasi M, Ebsworth Peter, Sugiarto Paulus, Anstey Nicholas M, Tjitra Emiliana, Price Richard N
International Health Division, Menzies School of Health Research, Darwin, Australia.
Malar J. 2008 Aug 2;7:148. doi: 10.1186/1475-2875-7-148.
Multidrug resistance has emerged to both Plasmodium vivax and Plasmodium falciparum and yet the comparative epidemiology of these infections is poorly defined.
All laboratory-confirmed episodes of malaria in Timika, Papua, Indonesia, presenting to community primary care clinics and an inpatient facility were reviewed over a two-year period. In addition information was gathered from a house-to-house survey to quantify the prevalence of malaria and treatment-seeking behaviour of people with fever.
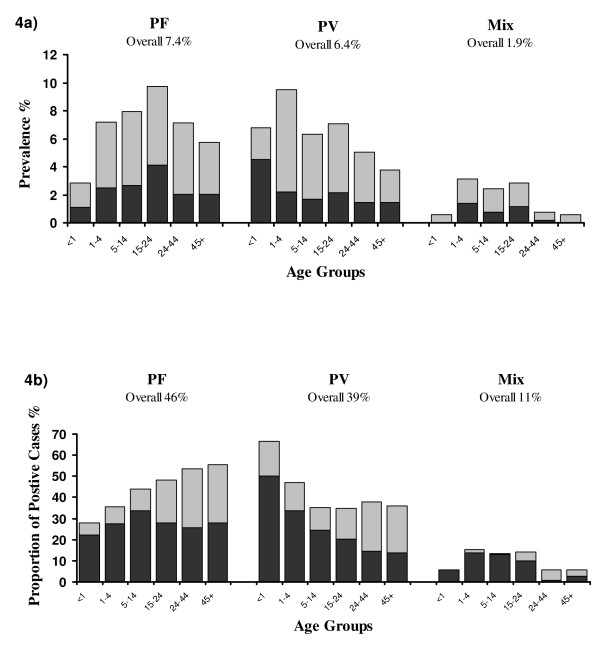
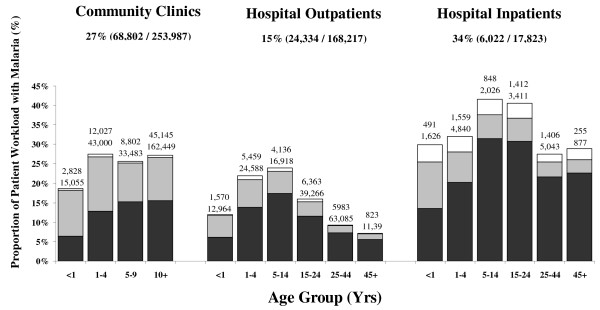
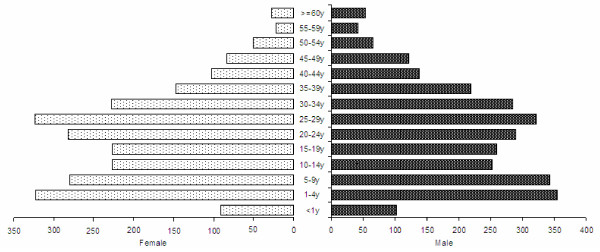
Between January 2004 and December 2005, 99,158 laboratory-confirmed episodes of malaria were reported, of which 58% (57,938) were attributable to P. falciparum and 37% (36,471) to P. vivax. Malaria was most likely to be attributable to pure P. vivax in children under one year of age (55% 2,684/4,889). In the household survey, the prevalence of asexual parasitaemia was 7.5% (290/3,890) for P. falciparum and 6.4% (248/3,890) for P. vivax. The prevalence of P. falciparum infection peaked in young adults aged 15-25 years (9.8% 69/707), compared to P. vivax infection which peaked in children aged 1 to 4 years (9.5% 61/642). Overall 35% (1,813/5,255) of people questioned reported a febrile episode in the preceding month. Of the 60% of people who were estimated to have had malaria, only 39% would have been detected by the surveillance network. The overall incidence of malaria was therefore estimated as 876 per 1,000 per year (Range: 711-906).
In this region of multidrug-resistant P. vivax and P. falciparum, both species are associated with substantial morbidity, but with significant differences in the age-related risk of infection.
间日疟原虫和恶性疟原虫均已出现多重耐药性,但这些感染的比较流行病学仍未明确界定。
对印度尼西亚巴布亚省蒂米卡社区基层医疗诊所和一家住院机构在两年期间所有实验室确诊的疟疾发作病例进行了回顾。此外,还通过挨家挨户调查收集信息,以量化疟疾患病率和发热患者的就医行为。
2004年1月至2005年12月期间,共报告了99,158例实验室确诊的疟疾发作病例,其中58%(57,938例)归因于恶性疟原虫,37%(36,471例)归因于间日疟原虫。一岁以下儿童的疟疾最有可能归因于单纯间日疟原虫感染(55%,2,684/4,889)。在家庭调查中,恶性疟原虫无性体血症患病率为7.5%(290/3,890),间日疟原虫为6.4%(248/3,890)。恶性疟原虫感染患病率在15至25岁的年轻人中达到峰值(9.8%,69/707),而间日疟原虫感染在1至4岁儿童中达到峰值(9.5%,61/642)。总体而言,35%(1,813/5,255)的受访者报告前一个月有发热发作。在估计患有疟疾的60%的人群中,监测网络仅能检测到39%。因此,疟疾的总体发病率估计为每年每1000人中有876例(范围:711 - 906)。
在这个间日疟原虫和恶性疟原虫均具有多重耐药性的地区,这两种疟原虫都与大量发病相关,但在年龄相关的感染风险方面存在显著差异。