Willison Donald J, Swinton Marilyn, Schwartz Lisa, Abelson Julia, Charles Cathy, Northrup David, Cheng Ji, Thabane Lehana
Department of Clinical Epidemiology & Biostatistics, McMaster University, Hamilton, Canada.
BMC Med Ethics. 2008 Nov 19;9:18. doi: 10.1186/1472-6939-9-18.
The role of consent for research use of health information is contentious. Most discussion has focused on when project-specific consent may be waived but, recently, a broader range of consent options has been entertained, including broad opt-in for multiple studies with restrictions and notification with opt-out. We sought to elicit public values in this matter and to work toward an agreement about a common approach to consent for use of personal information for health research through deliberative public dialogues.
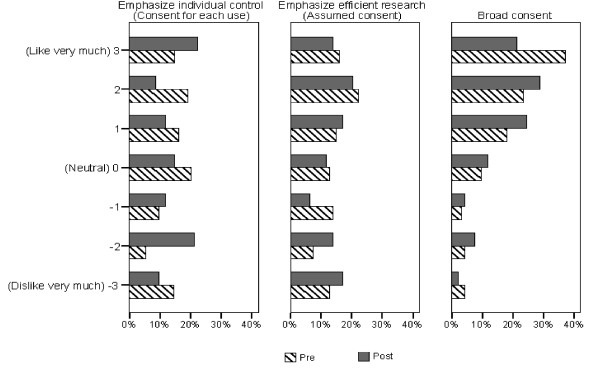
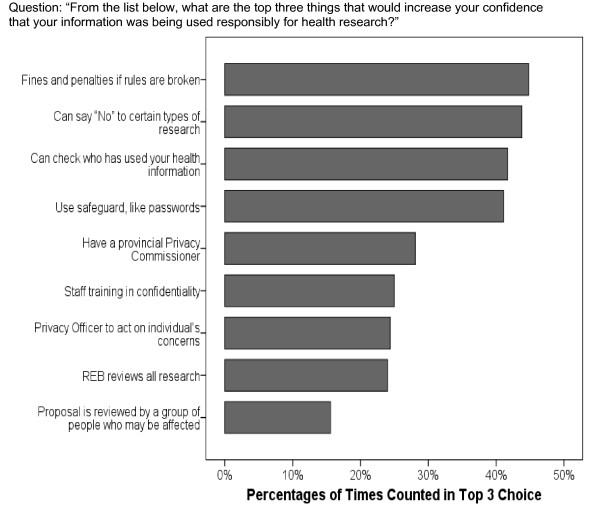
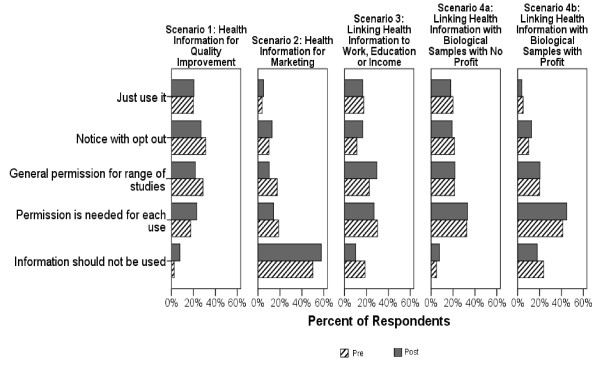
We conducted seven day-long public dialogues, involving 98 participants across Canada. Immediately before and after each dialogue, participants completed a fixed-response questionnaire rating individuals' support for 3 approaches to consent in the abstract and their consent choices for 5 health research scenarios using personal information. They also rated how confident different safeguards made them feel that their information was being used responsibly.
Broad opt-in consent for use of personal information garnered the greatest support in the abstract. When presented with specific research scenarios, no one approach to consent predominated. When profit was introduced into the scenarios, consent choices shifted toward greater control over use. Despite lively and constructive dialogues, and considerable shifting in opinion at the individual level, at the end of the day, there was no substantive aggregate movement in opinion. Personal controls were among the most commonly cited approaches to improving people's confidence in the responsible use of their information for research.
Because no one approach to consent satisfied even a simple majority of dialogue participants and the importance placed on personal controls, a mechanism should be developed for documenting consent choice for different types of research, including ways for individuals to check who has accessed their medical record for purposes other than clinical care. This could be done, for example, through a web-based patient portal to their electronic health record. Researchers and policy makers should continue to engage the public to promote greater public understanding of the research process and to look for feasible alternatives to existing approaches to project-specific consent for observational research.
健康信息用于研究的同意问题颇具争议。大多数讨论都集中在何时可以免除针对特定项目的同意,但最近,人们考虑了更广泛的同意选项,包括对多项研究的广泛选择加入(附带限制条件)以及选择退出的通知方式。我们试图在这个问题上引出公众的价值观,并通过公开的审议性对话,就健康研究中使用个人信息的同意通用方法达成共识。
我们开展了为期七天的公开对话,加拿大各地共有98名参与者。在每次对话前后,参与者都要完成一份固定答案问卷,对个人在抽象层面上对三种同意方法的支持程度,以及在使用个人信息的五种健康研究场景中的同意选择进行评分。他们还要对不同的保障措施让他们对自己的信息得到负责任使用的信心程度进行评分。
在抽象层面上,对使用个人信息的广泛选择加入同意获得了最大支持。当面对具体的研究场景时,没有一种同意方法占主导地位。当在场景中引入利润因素时,同意选择转向对使用有更大控制权。尽管对话热烈且富有建设性,个人层面的意见也有相当大的转变,但最终,总体意见并没有实质性的变化。个人控制是提高人们对其信息用于研究的负责任使用的信心的最常提及的方法之一。
由于没有一种同意方法能让哪怕简单多数的对话参与者满意,且人们对个人控制很重视,所以应该建立一种机制,用于记录不同类型研究的同意选择,包括个人检查谁出于临床护理以外的目的访问了他们的病历的方式。例如,可以通过基于网络的患者电子健康记录门户来实现。研究人员和政策制定者应继续与公众互动,以促进公众对研究过程有更深入的理解,并寻找现有观察性研究特定项目同意方法的可行替代方案。