van den Berg Gert, Abu-Issa Radwan, de Boer Bouke A, Hutson Mary R, de Boer Piet A J, Soufan Alexandre T, Ruijter Jan M, Kirby Margaret L, van den Hoff Maurice J B, Moorman Antoon F M
Heart Failure Research Center, Academic Medical Center, Amsterdam, The Netherlands.
Circ Res. 2009 Jan 30;104(2):179-88. doi: 10.1161/CIRCRESAHA.108.185843. Epub 2008 Dec 4.
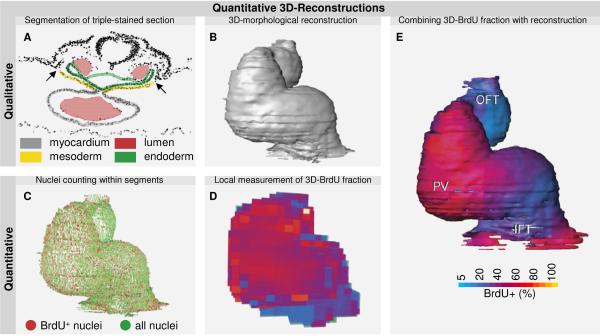
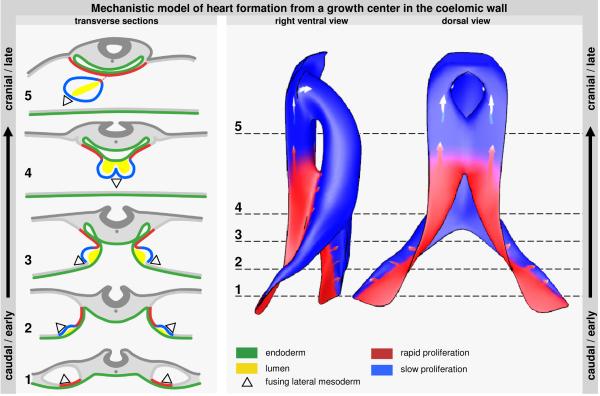
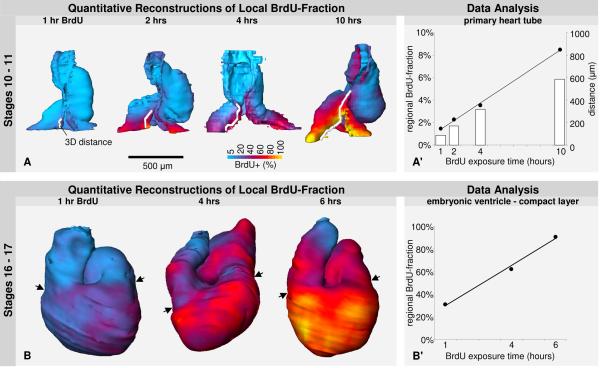
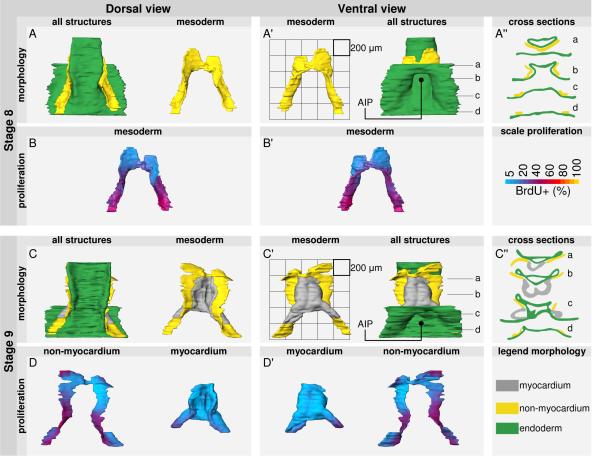
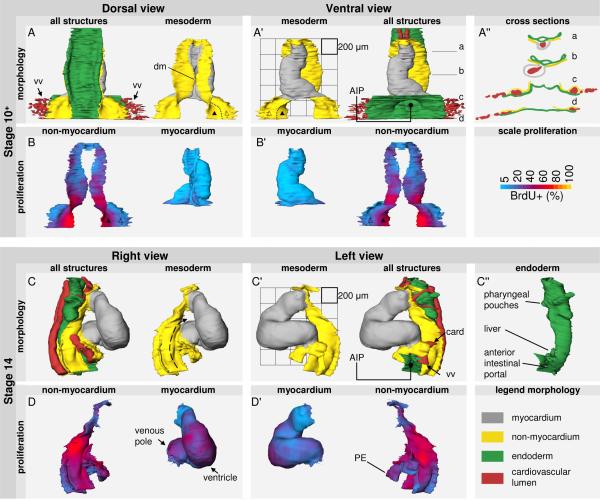
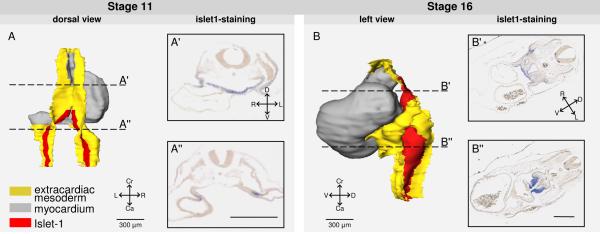
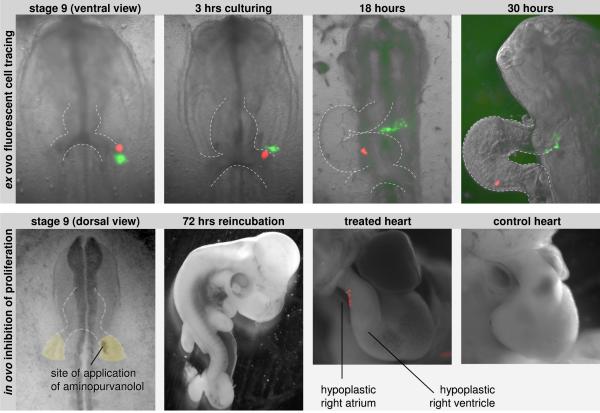
Recent studies have shown that the primary heart tube continues to grow by addition of cells from the coelomic wall. This growth occurs concomitantly with embryonic folding and formation of the coelomic cavity, making early heart formation morphologically complex. A scarcity of data on localized growth parameters further hampers the understanding of cardiac growth. Therefore, we investigated local proliferation during early heart formation. Firstly, we determined the cell cycle length of primary myocardium of the early heart tube to be 5.5 days, showing that this myocardium is nonproliferating and implying that initial heart formation occurs solely by addition of cells. In line with this, we show that the heart tube rapidly lengthens at its inflow by differentiation of recently divided precursor cells. To track the origin of these cells, we made quantitative 3D reconstructions of proliferation in the forming heart tube and the mesoderm of its flanking coelomic walls. These reconstructions show a single, albeit bilateral, center of rapid proliferation in the caudomedial pericardial back wall. This center expresses Islet1. Cell tracing showed that cells from this caudal growth center, besides feeding into the venous pole of the heart, also move cranially via the dorsal pericardial mesoderm and differentiate into myocardium at the arterial pole. Inhibition of caudal proliferation impairs the formation of both the atria and the right ventricle. These data show how a proliferating growth center in the caudal coelomic wall elongates the heart tube at both its venous and arterial pole, providing a morphological mechanism for early heart formation.
最近的研究表明,原始心管通过添加来自体腔壁的细胞而持续生长。这种生长与胚胎折叠和体腔的形成同时发生,使得早期心脏形成在形态学上变得复杂。关于局部生长参数的数据匮乏进一步阻碍了对心脏生长的理解。因此,我们研究了早期心脏形成过程中的局部增殖情况。首先,我们确定早期心管的原始心肌细胞周期长度为5.5天,这表明该心肌不增殖,意味着最初的心脏形成仅通过细胞添加来实现。与此一致的是,我们发现心管在其流入端通过最近分裂的前体细胞的分化而迅速延长。为了追踪这些细胞的起源,我们对正在形成的心管及其侧翼体腔壁的中胚层中的增殖情况进行了定量三维重建。这些重建显示在尾内侧心包后壁有一个单一的(尽管是双侧的)快速增殖中心。这个中心表达Islet1。细胞追踪显示,来自这个尾侧生长中心的细胞,除了进入心脏的静脉极外,还通过背侧心包中胚层向头侧移动,并在动脉极分化为心肌。抑制尾侧增殖会损害心房和右心室的形成。这些数据表明尾侧体腔壁中的一个增殖生长中心如何在心脏管的静脉极和动脉极使其延长,为早期心脏形成提供了一种形态学机制。