Sulman Erik P, Komaki Ritsuko, Klopp Ann H, Cox James D, Chang Joe Y
Department of Radiation Oncology, the University of Texas M, D, Anderson Cancer Center, 1515 Holcombe Boulevard, Houston, TX, USA.
Radiat Oncol. 2009 Jan 30;4:5. doi: 10.1186/1748-717X-4-5.
Controversy still exists regarding the long-term outcome of patients whose uninvolved lymph node stations are not prophylactically irradiated for non-small cell lung cancer (NSCLC) treated with definitive radiotherapy. To determine the frequency of elective nodal failure (ENF) and in-field failure (IFF), we examined a large cohort of patients with NSCLC staged with positron emission tomography (PET)/computed tomography (CT) and treated with 3-dimensional conformal radiotherapy (3D-CRT) that excluded uninvolved lymph node stations.
We retrospectively reviewed the records of 115 patients with non-small cell lung cancer treated at our institution with definitive radiation therapy with or without concurrent chemotherapy (CHT). All patients were treated with 3D-CRT, including nodal regions determined by CT or PET to be disease involved. Concurrent platinum-based CHT was administered for locally advanced disease. Patients were analyzed in follow-up for survival, local regional recurrence, and distant metastases (DM).
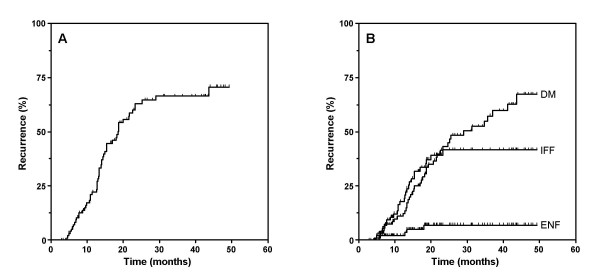
The median follow-up time was 18 months (3 to 44 months) among all patients and 27 months (6 to 44 months) among survivors. The median overall survival, 2-year actuarial overall survival and disease-free survival were 19 months, 38%, and 28%, respectively. The majority of patients died from DM, the overall rate of which was 36%. Of the 31 patients with local regional failure, 26 (22.6%) had IFF, 5 (4.3%) had ENF and 2 (1.7%) had isolated ENF. For 88 patients with stage IIIA/B, the frequencies of IFF, any ENF, isolated ENF, and DM were 23 (26%), 3 (9%), 1 (1.1%) and 36 (40.9%), respectively. The comparable rates for the 22 patients with early stage node-negative disease (stage IA/IB) were 3 (13.6%), 1(4.5%), 0 (0%), and 5 (22.7%), respectively.
We observed only a 4.3% recurrence of any ENF and a 1.7% recurrence of isolated ENF in patients with NSCLC treated with definitive 3D-CRT without prophylactic irradiation of uninvolved lymph node stations. Thus, distant metastasis and IFF remain the primary causes of treatment failure and cancer death in such patients, suggesting little value of ENI in this cohort.
对于接受根治性放疗的非小细胞肺癌(NSCLC)患者,其未受累淋巴结区域未进行预防性放疗的长期预后仍存在争议。为了确定选择性淋巴结失败(ENF)和野内失败(IFF)的发生率,我们研究了一大群经正电子发射断层扫描(PET)/计算机断层扫描(CT)分期并接受三维适形放疗(3D-CRT)且未包括未受累淋巴结区域的NSCLC患者。
我们回顾性分析了在我院接受根治性放疗(联合或不联合同步化疗)的115例非小细胞肺癌患者的记录。所有患者均接受3D-CRT治疗,包括由CT或PET确定为疾病累及的淋巴结区域。对于局部晚期疾病,给予基于铂的同步化疗。对患者进行随访,分析其生存、局部区域复发和远处转移(DM)情况。
所有患者的中位随访时间为18个月(3至44个月),存活患者的中位随访时间为27个月(6至44个月)。中位总生存期、2年精算总生存率和无病生存率分别为19个月、38%和28%。大多数患者死于DM,其总发生率为36%。在31例局部区域失败的患者中,26例(22.6%)发生IFF,5例(4.3%)发生ENF,2例(1.7%)发生孤立性ENF。对于88例IIIA/B期患者,IFF、任何ENF、孤立性ENF和DM的发生率分别为23例(26%)、3例(9%)、1例(1.1%)和36例(40.9%)。22例早期淋巴结阴性疾病(IA/IB期)患者的相应发生率分别为3例(13.6%)、1例(4.5%)、0例(0%)和5例(22.7%)。
在未对未受累淋巴结区域进行预防性放疗而接受根治性3D-CRT治疗的NSCLC患者中,我们观察到任何ENF的复发率仅为4.3%,孤立性ENF的复发率为1.7%。因此,远处转移和IFF仍然是这类患者治疗失败和癌症死亡的主要原因,提示在该队列中ENI的价值不大。