Fitzpatrick Annette L, Kuller Lewis H, Lopez Oscar L, Diehr Paula, O'Meara Ellen S, Longstreth W T, Luchsinger José A
Department of Epidemiology, University of Washington, Collaborative Health Studies Coordinating Center, Seattle, 98115, USA.
Arch Neurol. 2009 Mar;66(3):336-42. doi: 10.1001/archneurol.2008.582.
While high adiposity in middle age appears to be related to greater dementia risk, studies exploring this association in the elderly are conflicting.
To evaluate associations between midlife and late-life obesity and risk of dementia.
Prospective study with mean follow-up of 5.4 years (1992-1994 through 1999).
Community-dwelling sample in 4 US sites recruited from Medicare eligibility files.
A total of 2798 adults without dementia (mean age, 74.7 years; 59.1% women) participating in the Cardiovascular Health Study who underwent magnetic resonance imaging were measured for height and weight at baseline at age 65 years or older (late life), and self-reported weight at age 50 years (midlife). Body mass index (BMI) (calculated as weight in kilograms divided by height in meters squared) was calculated at both times.
Dementia, Alzheimer disease, and vascular dementia classified by a multidisciplinary committee using standardized criteria.
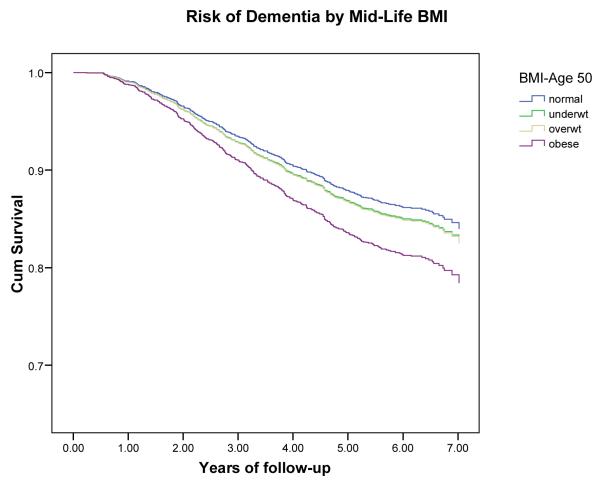
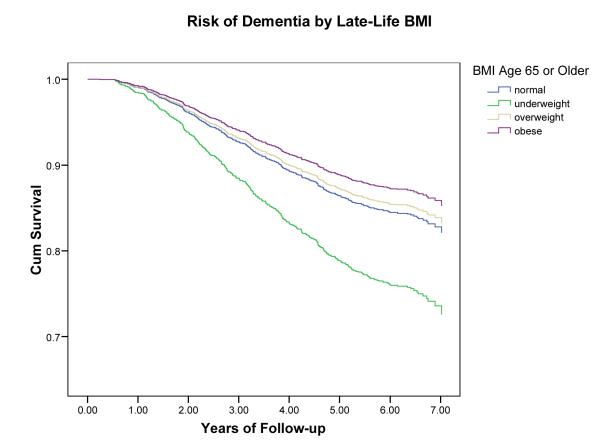
Classification resulted in 480 persons with incident dementia, 245 with Alzheimer disease (no vascular dementia), and 213 with vascular dementia (with or without Alzheimer disease). In evaluations of midlife obesity, an increased risk of dementia was found for obese (BMI >30) vs normal-weight (BMI 20-25) persons, adjusted for demographics (hazard ratio [HR], 1.39; 95% confidence interval [CI], 1.03-1.87) and for cardiovascular risk factors (1.36; 0.94-1.95). The risk estimates were reversed in assessments of late-life BMI. Underweight persons (BMI <20) had an increased risk of dementia (1.62; 1.02-2.64), whereas being overweight (BMI >25-30) was not associated (0.92; 0.72-1.18) and being obese reduced the risk of dementia (0.63; 0.44-0.91) compared with those with normal BMI.
These results help explain the "obesity paradox" as differences in dementia risk across time are consistent with physical changes in the trajectory toward disability.
虽然中年时期的高肥胖程度似乎与更高的痴呆风险相关,但在老年人中探索这种关联的研究结果相互矛盾。
评估中年和晚年肥胖与痴呆风险之间的关联。
前瞻性研究,平均随访5.4年(1992 - 1994年至1999年)。
从医疗保险资格档案中招募的美国4个地点的社区居住样本。
共有2798名无痴呆的成年人(平均年龄74.7岁;59.1%为女性)参与心血管健康研究,这些人在65岁及以上(晚年)的基线时接受了磁共振成像检查,并测量了身高和体重,同时报告了50岁(中年)时的自我体重。两次均计算了体重指数(BMI)(计算方法为体重千克数除以身高米数的平方)。
由多学科委员会使用标准化标准分类的痴呆、阿尔茨海默病和血管性痴呆。
分类结果显示,有480人发生痴呆,245人患阿尔茨海默病(无血管性痴呆),213人患血管性痴呆(有或无阿尔茨海默病)。在对中年肥胖的评估中,发现肥胖(BMI>30)者与正常体重(BMI 20 - 25)者相比,痴呆风险增加,经人口统计学因素调整后(风险比[HR],1.39;95%置信区间[CI],1.03 - 1.87)以及经心血管危险因素调整后(1.36;0.94 - 1.95)。在对晚年BMI的评估中,风险估计值相反。体重过轻(BMI<20)者患痴呆的风险增加(1.62;1.02 - 2.64),而超重(BMI>25 - 30)者无关联(0.92;0.72 - 1.18),与BMI正常者相比,肥胖者患痴呆的风险降低(0.63;0.44 - 0.91)。
这些结果有助于解释“肥胖悖论”,因为不同时间的痴呆风险差异与向残疾发展轨迹中的身体变化一致。