Nieder Carsten, Marienhagen Kirsten, Astner Sabrina T, Molls Michael
Radiation Oncology Unit, Nordlandssykehuset HF, Bodø, Norway.
BMC Cancer. 2009 Apr 7;9:105. doi: 10.1186/1471-2407-9-105.
Prognostic scores might be useful tools both in clinical practice and clinical trials, where they can be used as stratification parameter. The available scores for patients with brain metastases have never been tested specifically in patients with primary breast cancer. It is therefore unknown which score is most appropriate for these patients.
Five previously published prognostic scores were evaluated in a group of 83 patients with brain metastases from breast cancer. All patients had been treated with whole-brain radiotherapy with or without radiosurgery or surgical resection. In addition, it was tested whether the parameters that form the basis of these scores actually have a prognostic impact in this biologically distinct group of brain metastases patients.
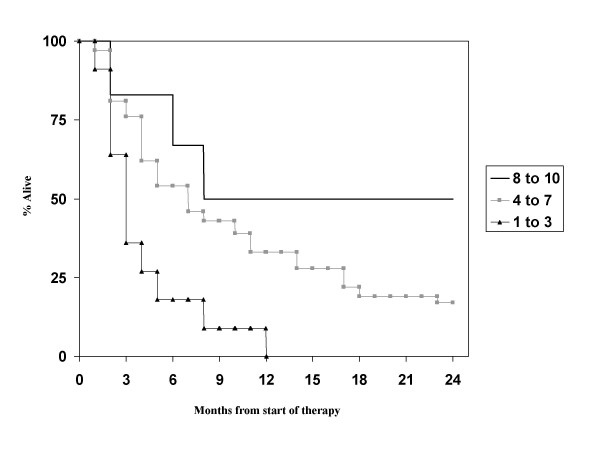
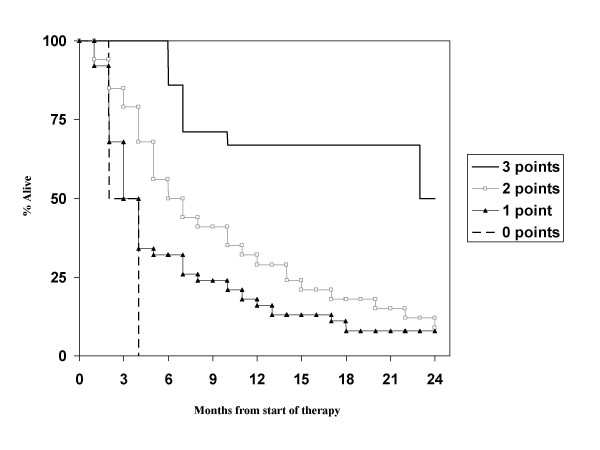
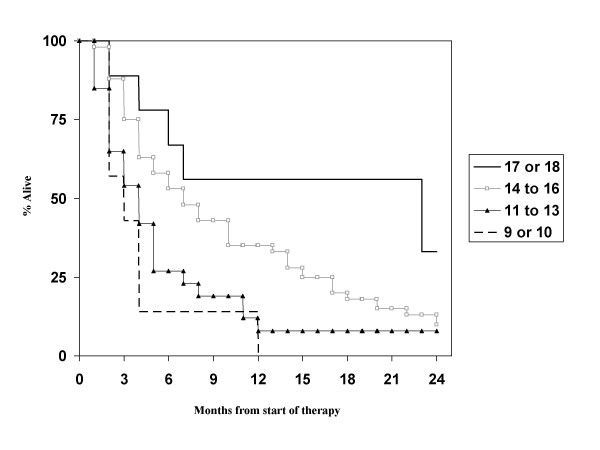
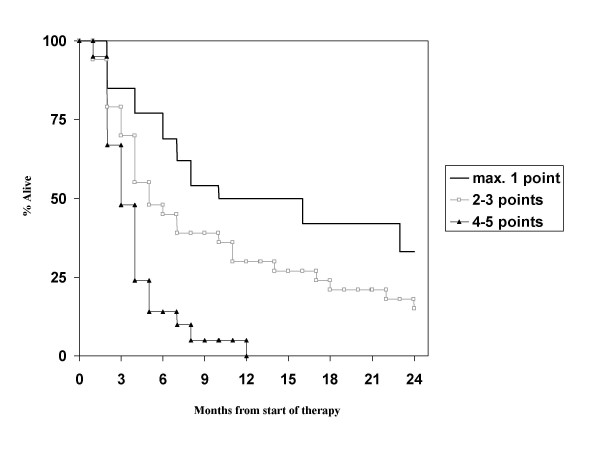
The scores that performed best were the recursive partitioning analysis (RPA) classes and the score index for radiosurgery (SIR). However, disagreement between the parameters that form the basis of these scores and those that determine survival in the present group of patients and many reported data from the literature on brain metastases from breast cancer was found. With the four statistically significant prognostic factors identified here, a 3-tiered score can be created that performs slightly better than RPA and SIR. In addition, a 4-tiered score is also possible, which performs better than the three previous 4-tiered scores, incl. graded prognostic assessment (GPA) score and basic score for brain metastases (BSBM).
A variety of prognostic models describe the survival of patients with brain metastases from breast cancer to a more or less satisfactory degree. However, the standard brain metastases scores might not fully appreciate the unique biology and time course of this disease, e.g., compared to lung cancer. It appears possible that inclusion of emerging prognostic factors will improve the results and allow for development and validation of a consensus score for broad clinical application. The model that is based on the authors own patient group, which is not large enough to fully evaluate a large number of potential prognostic factors, is meant to illustrate this point rather than to provide the definitive score.
预后评分在临床实践和临床试验中可能都是有用的工具,可作为分层参数。现有的脑转移患者评分从未在原发性乳腺癌患者中进行过专门测试。因此,尚不清楚哪种评分最适合这些患者。
在一组83例乳腺癌脑转移患者中评估了5种先前发表的预后评分。所有患者均接受了全脑放疗,部分患者还接受了放射外科手术或手术切除。此外,还测试了构成这些评分基础的参数在这一生物学特性不同的脑转移患者群体中是否真的具有预后影响。
表现最佳的评分是递归分区分析(RPA)类别和放射外科手术评分指数(SIR)。然而,发现构成这些评分基础的参数与本研究组中决定生存的参数之间存在分歧,并且与许多乳腺癌脑转移文献报道的数据也存在分歧。利用这里确定的4个具有统计学意义的预后因素,可以创建一个3级评分,其表现略优于RPA和SIR。此外,也可以创建一个4级评分,其表现优于之前的3个4级评分,包括分级预后评估(GPA)评分和脑转移基础评分(BSBM)。
多种预后模型对乳腺癌脑转移患者的生存情况或多或少地进行了令人满意的描述。然而,标准的脑转移评分可能无法充分认识到这种疾病独特的生物学特性和病程,例如与肺癌相比。纳入新出现的预后因素似乎有可能改善结果,并有助于开发和验证一个广泛临床应用的共识评分。基于作者自己患者群体的模型,由于规模不足以全面评估大量潜在的预后因素,旨在说明这一点,而不是提供最终评分。