Zolopa Andrew, Andersen Janet, Powderly William, Sanchez Alejandro, Sanne Ian, Suckow Carol, Hogg Evelyn, Komarow Lauren
Stanford University AIDS Clinical Trials Unit, Stanford University, Stanford, California, United States of America.
PLoS One. 2009;4(5):e5575. doi: 10.1371/journal.pone.0005575. Epub 2009 May 18.
Optimal timing of ART initiation for individuals presenting with AIDS-related OIs has not been defined.
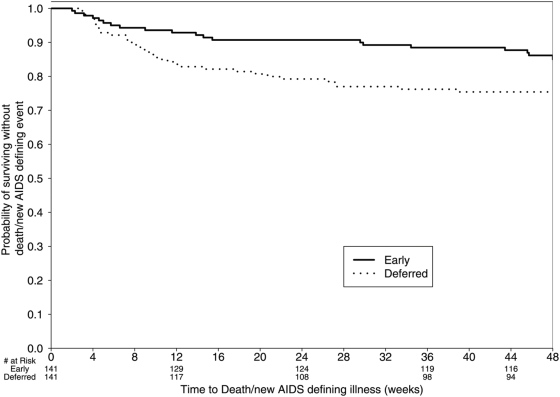
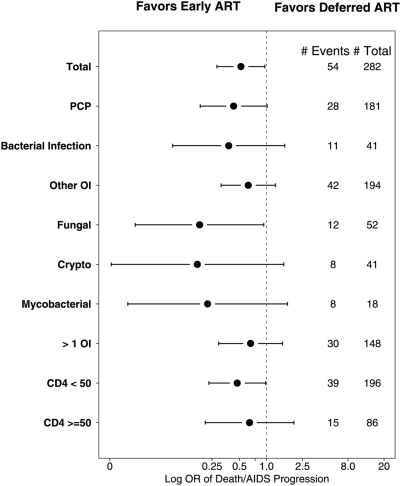
A5164 was a randomized strategy trial of "early ART"--given within 14 days of starting acute OI treatment versus "deferred ART"--given after acute OI treatment is completed. Randomization was stratified by presenting OI and entry CD4 count. The primary week 48 endpoint was 3-level ordered categorical variable: 1. Death/AIDS progression; 2. No progression with incomplete viral suppression (ie HIV viral load (VL) >or=50 copies/ml); 3. No progression with optimal viral suppression (ie HIV VL <50 copies/ml). Secondary endpoints included: AIDS progression/death; plasma HIV RNA and CD4 responses and safety parameters including IRIS. 282 subjects were evaluable; 141 per arm. Entry OIs included Pneumocytis jirovecii pneumonia 63%, cryptococcal meningitis 12%, and bacterial infections 12%. The early and deferred arms started ART a median of 12 and 45 days after start of OI treatment, respectively. THE DIFFERENCE IN THE PRIMARY ENDPOINT DID NOT REACH STATISTICAL SIGNIFICANCE: AIDS progression/death was seen in 20 (14%) vs. 34 (24%); whereas no progression but with incomplete viral suppression was seen in 54 (38%) vs. 44 (31%); and no progression with optimal viral suppression in 67 (48%) vs 63 (45%) in the early vs. deferred arm, respectively (p = 0.22). However, the early ART arm had fewer AIDS progression/deaths (OR = 0.51; 95% CI = 0.27-0.94) and a longer time to AIDS progression/death (stratified HR = 0.53; 95% CI = 0.30-0.92). The early ART had shorter time to achieving a CD4 count above 50 cells/mL (p<0.001) and no increase in adverse events.
Early ART resulted in less AIDS progression/death with no increase in adverse events or loss of virologic response compared to deferred ART. These results support the early initiation of ART in patients presenting with acute AIDS-related OIs, absent major contraindications.
ClinicalTrials.gov NCT00055120.
对于患有艾滋病相关机会性感染(OI)的个体,抗逆转录病毒治疗(ART)开始的最佳时机尚未明确。
A5164是一项随机策略试验,比较“早期ART”(在急性OI治疗开始后14天内给予)与“延迟ART”(在急性OI治疗完成后给予)。随机分组按所患OI和入组时的CD4细胞计数进行分层。第48周的主要终点是一个三级有序分类变量:1. 死亡/艾滋病进展;2. 无进展但病毒抑制不完全(即HIV病毒载量(VL)≥50拷贝/ml);3. 无进展且病毒得到最佳抑制(即HIV VL<50拷贝/ml)。次要终点包括:艾滋病进展/死亡;血浆HIV RNA和CD4细胞反应以及包括免疫重建炎症综合征(IRIS)在内的安全性参数。282名受试者可进行评估,每组141名。入组时的OI包括耶氏肺孢子菌肺炎63%、隐球菌性脑膜炎12%和细菌感染12%。早期治疗组和延迟治疗组分别在OI治疗开始后的中位数12天和45天开始ART。主要终点的差异未达到统计学显著性:早期治疗组和延迟治疗组出现艾滋病进展/死亡的分别为20例(14%)和34例(24%);无进展但病毒抑制不完全的分别为54例(38%)和44例(31%);无进展且病毒得到最佳抑制的分别为67例(48%)和63例(45%)(p = 0.22)。然而,早期ART组的艾滋病进展/死亡病例较少(比值比 = 0.51;95%置信区间 = 0.27 - 0.94),且至艾滋病进展/死亡的时间更长(分层风险比 = 0.53;95%置信区间 = 0.30 - 0.92)。早期ART组达到CD4细胞计数高于50个细胞/ml的时间更短(p<0.001),且不良事件没有增加。
与延迟ART相比,早期ART导致艾滋病进展/死亡更少,不良事件没有增加,病毒学反应也没有丧失。这些结果支持在没有主要禁忌证的情况下,对患有急性艾滋病相关OI的患者尽早开始ART。
ClinicalTrials.gov NCT00055120