Department of Anesthesiology and Intensive Care Medicine, University Hospital Muenster, Albert-Schweitzer-Str, 33, 48149 Muenster, Germany.
Crit Care. 2009;13(4):R109. doi: 10.1186/cc7950. Epub 2009 Jul 6.
Increasing evidence indicates that epidural anesthesia improves postoperative pulmonary function. The underlying mechanisms, however, remain to be determined. Because pulmonary nitric oxide has been identified to play a critical role in pulmonary dysfunction in sepsis, we hypothesized that thoracic epidural anesthesia (TEA) modulates endothelial dysfunction via a nitric oxide-dependent pathway.
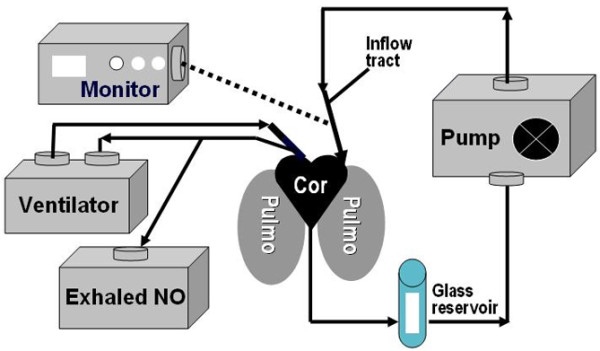
Thirty-six Sprague-Dawley rats underwent sham laparotomy or induction of peritoneal sepsis caused by cecal ligation and puncture (CLP). Septic animals were then treated with either bupivacaine 0.5% or normal saline epidurally (15 microl/h-1) for 6 hours or 24 hours after injury. Previous experiments demonstrated that these time points correspond with a hyperdynamic (at 6 hours) and hypodynamic circulation (at 24 hours), respectively. In addition, two sham control groups received either bupivacaine 0.5% or normal saline epidurally (15 microl/h-1). Six and 24 hours after injury, hemodynamic measurements and arterial blood gas analyses were performed in awake, spontaneously breathing rats. Exhaled nitric oxide, bradykinin-induced pulmonary vasoconstriction (a surrogate marker of endothelial dysfunction), pulmonary wet/dry-weight ratio (an estimate of pulmonary edema), and myeloperoxidase activity (MPO, a surrogate marker of neutrophil infiltration into lung tisssue) were investigated at 6 and 24 hours by using an established model of isolated and perfused lungs.
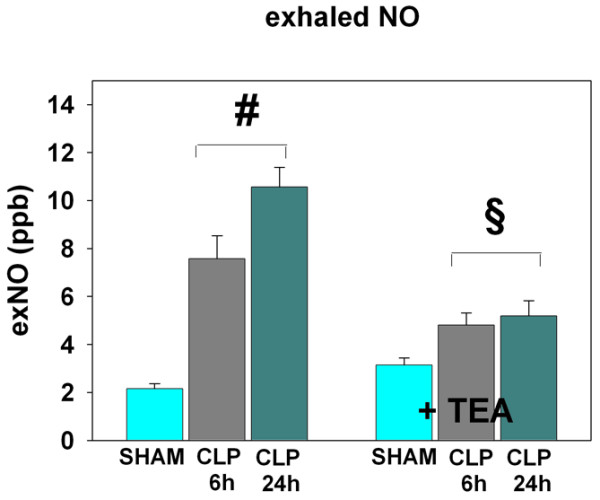
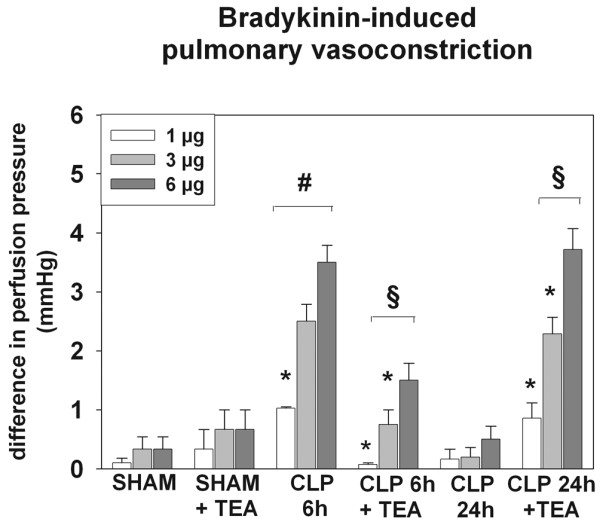
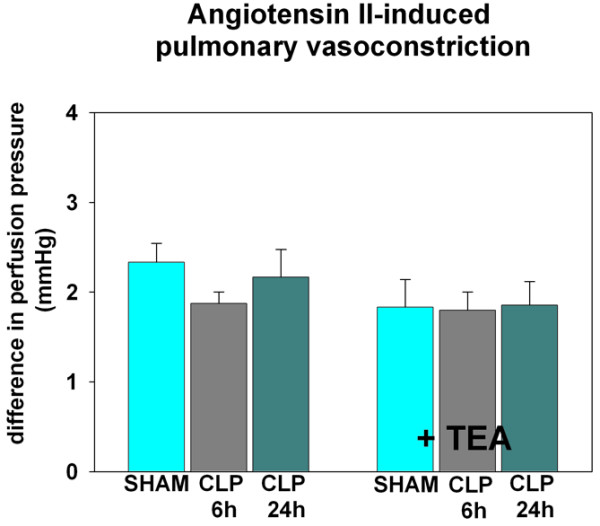
In hyperdynamic sepsis, treatment with TEA resulted in reduced bradykinin-induced pulmonary vasoconstriction (P < 0.05) and lower levels of exhaled NO as compared with those in untreated septic rats (P < 0.05). However, the development of pulmonary edema or MPO activity in the lungs was not alleviated by sympathetic blockade in this phase of sepsis. Conversely, TEA led to an increased bradykinin-induced pulmonary vasoconstriction and pulmonary edema despite reduced exNO levels and pulmonary MPO activity in hypodynamic sepsis (each P < 0.05 versus CLP 24 h). Pulmonary gas exchange was only marginally affected under the influence of TEA in hypodynamic sepsis. Mean arterial pressure and heart rate were not affected beyond the changes caused by sepsis itself.
The results of the present study suggest that TEA modulates the NO pathway and exerts positive effects on pulmonary endothelial integrity only in hyperdynamic sepsis. Whether the negative effects on endothelial function in hypodynamic sepsis have an impact on overall morbidity and mortality remains to be determined in future studies.
越来越多的证据表明,硬膜外麻醉可改善术后肺功能。然而,其潜在机制尚待确定。由于已发现肺一氧化氮在脓毒症导致的肺功能障碍中起关键作用,我们假设胸段硬膜外麻醉(TEA)通过一氧化氮依赖途径调节内皮功能障碍。
36 只 Sprague-Dawley 大鼠接受假手术或盲肠结扎穿刺(CLP)诱导的腹膜脓毒症。然后,在损伤后 6 小时或 24 小时,用布比卡因 0.5%或生理盐水硬膜外(15 微升/小时-1)治疗败血症动物。先前的实验表明,这些时间点分别对应于高动力(6 小时)和低动力循环(24 小时)。此外,两个假对照大鼠组分别接受布比卡因 0.5%或生理盐水硬膜外(15 微升/小时-1)。损伤后 6 小时和 24 小时,在清醒、自主呼吸的大鼠中进行血流动力学测量和动脉血气分析。使用已建立的离体灌注肺模型,在 6 小时和 24 小时时,通过测量呼气一氧化氮(exhaled nitric oxide,NO)、缓激肽诱导的肺血管收缩(内皮功能障碍的替代标志物)、肺湿/干重比(肺水肿的估计值)和髓过氧化物酶活性(MPO,中性粒细胞浸润肺组织的替代标志物)来研究。
在高动力性脓毒症中,与未治疗的败血症大鼠相比(P<0.05),TEA 治疗可降低缓激肽诱导的肺血管收缩(P<0.05)和降低呼气一氧化氮(exhaled NO)水平。然而,在该阶段的脓毒症中,交感神经阻断并不能减轻肺内水肿或 MPO 活性的发展。相反,尽管在低动力性脓毒症中 exNO 水平和肺 MPO 活性降低,但 TEA 导致缓激肽诱导的肺血管收缩和肺水肿增加(与 CLP 24 h 相比,各 P<0.05)。在低动力性脓毒症中,TEA 的影响仅使肺气体交换略有变化。平均动脉压和心率不受脓毒症本身引起的变化以外的影响。
本研究结果表明,TEA 仅在高动力性脓毒症中调节一氧化氮途径并对肺内皮完整性产生积极影响。在低动力性脓毒症中,对内皮功能的负面影响是否会对整体发病率和死亡率产生影响,仍有待进一步研究确定。