Department of Radiology (HP E01.132), University Medical Center, P. O. Box 85500, 3508 GA, Utrecht, The Netherlands.
Neuroradiology. 2009 Dec;51(12):813-9. doi: 10.1007/s00234-009-0575-y. Epub 2009 Jul 22.
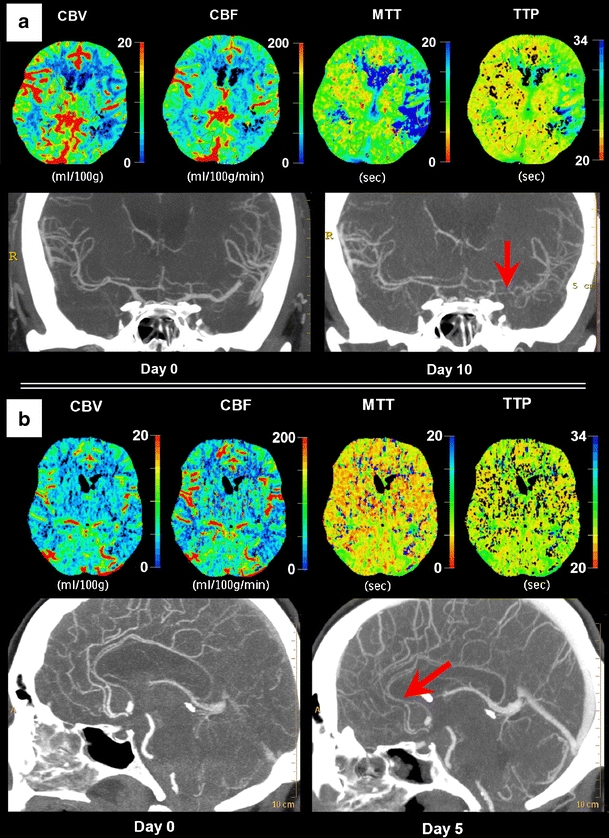
Vasospasm after aneurysmal subarachnoid hemorrhage (SAH) is thought to cause ischemia. To evaluate the contribution of vasospasm to delayed cerebral ischemia (DCI), we investigated the effect of vasospasm on cerebral perfusion and the relationship of vasospasm with DCI.
We studied 37 consecutive SAH patients with CT angiography (CTA) and CT perfusion (CTP) on admission and within 14 days after admission or at time of clinical deterioration. CTP values (cerebral blood volume, cerebral blood flow (CBF) and mean transit time), degree of vasospasm on CTA, and occurrence of DCI were recorded. Vasospasm was categorized as follows: no spasm (0-25% decrease in vessel diameter), moderate spasm (25-50% decrease), and severe spasm (>50% decrease). The correspondence of the flow territory of the most spastic vessel with the least perfused region was evaluated, and differences in perfusion values and occurrence of DCI between degrees of vasospasm were calculated with 95% confidence intervals (95% CI).
Fourteen patients had no vasospasm, 16 were moderate, and seven were severe. In 65% of patients with spasm, the flow territory of the most spastic vessel corresponded with the least perfused region. There was significant CBF (milliliters per 100 g per minute) difference (-21.3; 95% CI, -37 <--> -5.3) between flow territories of severe and no vasospasm. Four of seven patients with severe, six of 16 with moderate, and three of 14 patients with no vasospasm had DCI.
Vasospasm decreases cerebral perfusion, but corresponds with the least perfused region in only two thirds of our patients. Furthermore, almost half of patients with severe vasospasm do not have DCI. Thus, although severe vasospasm can decrease perfusion, it may not result in DCI.
人们认为,蛛网膜下腔出血(SAH)后的血管痉挛会导致缺血。为了评估血管痉挛对迟发性脑缺血(DCI)的影响,我们研究了血管痉挛对脑灌注的影响,以及血管痉挛与 DCI 的关系。
我们研究了 37 例连续的 SAH 患者,他们在入院时和入院后 14 天内或临床恶化时进行了 CT 血管造影(CTA)和 CT 灌注(CTP)检查。记录了 CTP 值(脑血容量、脑血流(CBF)和平均通过时间)、CTA 上的血管痉挛程度以及 DCI 的发生情况。血管痉挛分为:无痉挛(血管直径减少 0-25%)、中度痉挛(血管直径减少 25-50%)和重度痉挛(血管直径减少>50%)。评估最痉挛血管的血流区域与最灌注不足区域的对应关系,并计算不同程度血管痉挛之间的灌注值和 DCI 的发生率差异,置信区间为 95%(95%CI)。
14 例患者无血管痉挛,16 例为中度痉挛,7 例为重度痉挛。在 65%的痉挛患者中,最痉挛血管的血流区域与最灌注不足区域相对应。严重和无痉挛之间的 CBF(每分钟每 100 克毫升)差异有统计学意义(-21.3;95%CI,-37 <--> -5.3)。7 例重度痉挛患者中有 4 例、16 例中度痉挛患者中有 6 例、14 例无痉挛患者中有 3 例发生 DCI。
血管痉挛会降低脑灌注,但在我们的患者中只有三分之二的情况下与最灌注不足的区域相对应。此外,几乎一半的重度血管痉挛患者没有发生 DCI。因此,尽管重度血管痉挛会降低灌注,但它可能不会导致 DCI。