Cytokines & Inflammation Unit, Institut Pasteur, 28 rue Dr, Roux, 75015 Paris, France.
Crit Care. 2009;13(4):R124. doi: 10.1186/cc7980. Epub 2009 Jul 28.
The gut is often considered as the motor of critical illness through bacterial translocation, which amplifies the inflammatory response and alters the immune status. However, systemic bacterial translocation was rarely proven and endotoxin measurement only reflects translocation of Gram-negative-derived products. The process could be more frequently identified if peptidoglycan, derived from both Gram-negative and Gram-positive bacteria, was measured.
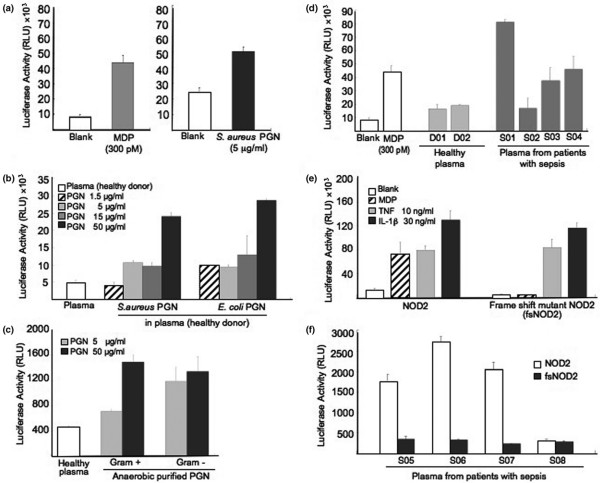
We developed a new tool to detect circulating peptidoglycan-like structure using a NOD2-transfected cell line. We also measured plasma and cell-associated endotoxin and different plasma markers of inflammation. We studied 21 patients undergoing abdominal aortic surgery (AAS), and 21 patients undergoing carotid artery surgery (CAS) were included as negative controls. Patients were sampled during surgery until two days post-surgery.
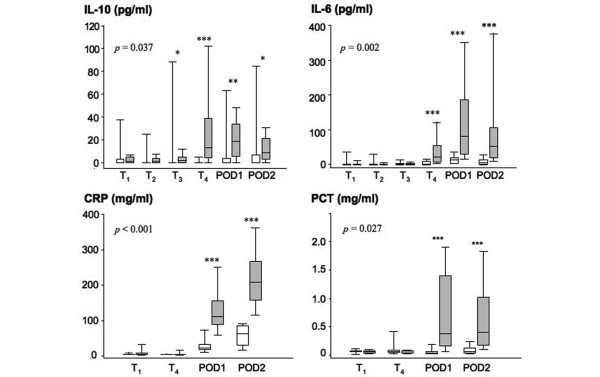
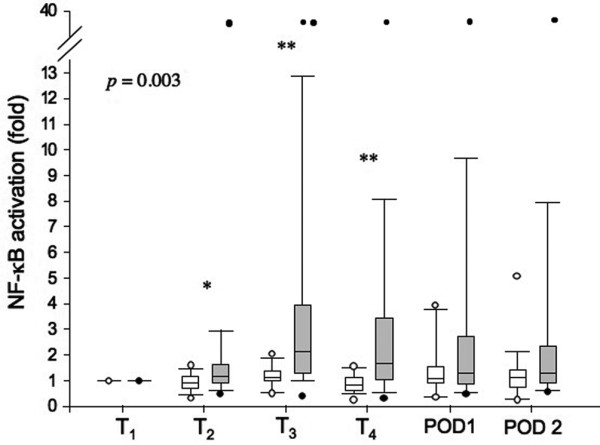
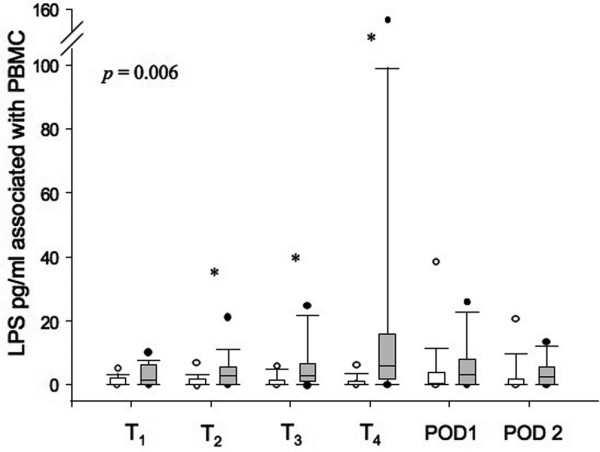
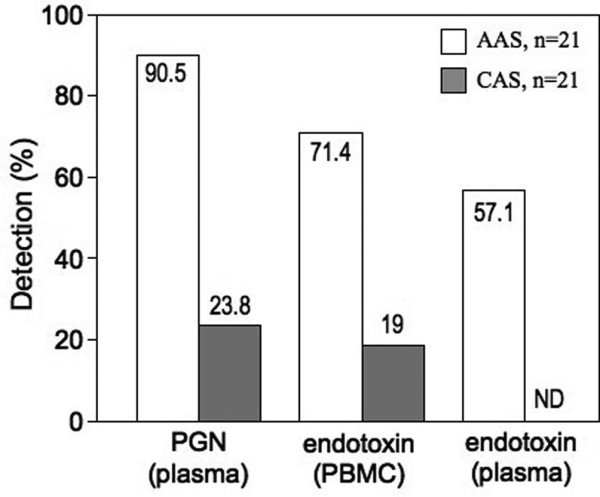
In 90.5% of the AAS patients, a NOD2 agonist peak was detected in plasma before aortic clamping, but after gut manipulation by the surgeon, and persisted after blood reperfusion. As expected, no peak was detected in plasma from CAS patients (P = 0.003). Leukocyte-bound endotoxin appeared after blood reperfusion in 71% of the AAS patients, and circulating endotoxin was detected for 57% of them. The levels of interleukin (IL)-6, IL-10 and of inflammatory markers (C-reactive protein, procalcitonin) were maximal at postoperative day 1 or 2 in AAS patients. The levels of circulating NOD2 agonist positively correlated with those of cortisol and IL-10.
The measurement of circulating NOD2 agonist gives a higher informative tool than that of circulating endotoxin for early and sensitive detection of the translocation of bacterial products. The data suggest that circulating NOD2 agonist contributes to further enhance the stress response following surgery.
肠道通常被认为是通过细菌易位引发危重病的动力,细菌易位会放大炎症反应并改变免疫状态。然而,全身细菌易位很少得到证实,内毒素测量仅反映革兰氏阴性衍生产物的易位。如果测量来源于革兰氏阴性和革兰氏阳性细菌的肽聚糖,那么这个过程可能会更频繁地被识别。
我们开发了一种使用 NOD2 转染细胞系检测循环肽聚糖样结构的新工具。我们还测量了血浆和细胞相关内毒素以及不同的炎症血浆标志物。我们研究了 21 例接受腹主动脉手术(AAS)的患者,21 例接受颈动脉手术(CAS)的患者作为阴性对照。患者在手术期间进行采样,直到术后两天。
在 90.5%的 AAS 患者中,在主动脉夹闭前的血浆中检测到 NOD2 激动剂峰值,但在外科医生进行肠道操作后,并在血液再灌注后持续存在。正如预期的那样,在 CAS 患者的血浆中未检测到峰值(P = 0.003)。白细胞结合内毒素在 71%的 AAS 患者中在血液再灌注后出现,并且在其中 57%的患者中检测到循环内毒素。AAS 患者的白细胞介素 (IL)-6、IL-10 和炎症标志物(C 反应蛋白、降钙素原)水平在术后第 1 天或第 2 天达到最大值。循环 NOD2 激动剂的水平与皮质醇和 IL-10 的水平呈正相关。
与循环内毒素相比,循环 NOD2 激动剂的测量为早期和敏感检测细菌产物的易位提供了更高的信息工具。这些数据表明,循环 NOD2 激动剂有助于进一步增强手术后的应激反应。