Ahmed Syed Masud, Haque Rashidul, Haque Ubydul, Hossain Awlad
BRAC Research and Evaluation Division, BRAC Centre, 75 Mohakhali, Dhaka-1212 Bangladesh.
Malar J. 2009 Jul 29;8:173. doi: 10.1186/1475-2875-8-173.
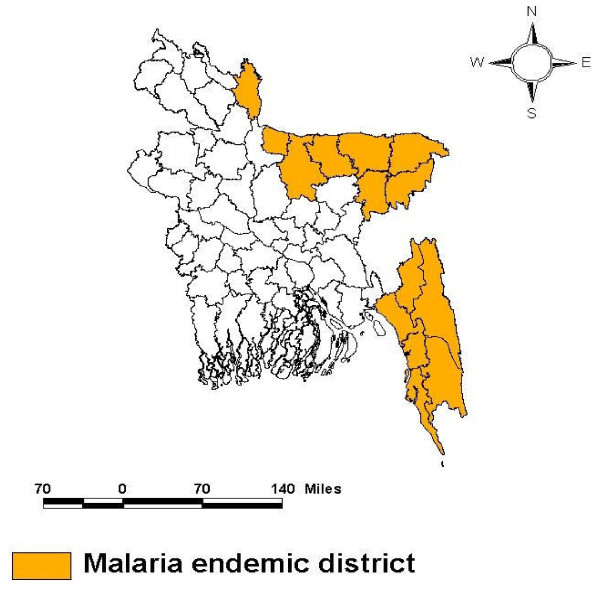
Data on sociological and behavioural aspects of malaria, which is essential for an evidence-based design of prevention and control programmes, is lacking in Bangladesh. This paper attempts to fill this knowledge gap by using data from a population-based prevalence survey conducted during July to November 2007, in 13 endemic districts of Bangladesh.
A two-stage cluster sampling technique was used to select study respondents randomly from 30 mauzas in each district for the socio-behavioural inquiry (n = 9,750). A pre-tested, semi-structured questionnaire was used to collect data in face-to-face interview by trained interviewers, after obtaining informed consent.
The overall malaria prevalence rate in the 13 endemic districts was found to be 3.1% by the Rapid Diagnostic Test 'FalciVax' (P. falciparum 2.73%, P. vivax 0.16% and mixed infection 0.19%), with highest concentration in the three hill districts (11%). Findings revealed superficial knowledge on malaria transmission, prevention and treatment by the respondents. Poverty and level of schooling were found as important determinants of malaria knowledge and practices. Allopathic treatment was uniformly advocated, but the 'know-do' gap became especially evident when in practice majority of the ill persons either did not seek any treatment (31%) or practiced self-treatment (12%). Of those who sought treatment, the majority went to the village doctors and drugstore salespeople (around 40%). Also, there was a delay beyond twenty-four hours in beginning treatment of malaria-like fever in more than half of the instances. In the survey, gender divide in knowledge and health-seeking behaviour was observed disfavouring women. There was also a geographical divide between the high endemic south-eastern area and the low-endemicnorth-eastern area, the former being disadvantaged with respect to different aspects of malaria studied.
The respondents in this study lacked comprehensive knowledge on different aspects of malaria, which was influenced by level of poverty and education. A gender and geographical divide in knowledge was observed disfavouring women and south-eastern area respectively. They preferred allopathic treatment for malaria, although a substantial proportion did not seek any treatment or sought self-treatment for malaria-like fever. Delay in seeking care was common. The implications of these findings for programme development are discussed.
孟加拉国缺乏有关疟疾社会学和行为学方面的数据,而这些数据对于循证设计预防和控制项目至关重要。本文试图通过使用2007年7月至11月期间在孟加拉国13个疟疾流行地区开展的一项基于人群的患病率调查数据来填补这一知识空白。
采用两阶段整群抽样技术,从每个地区的30个村庄中随机选取研究对象进行社会行为调查(n = 9750)。在获得知情同意后,由经过培训的访谈员使用预先测试的半结构化问卷,通过面对面访谈收集数据。
通过快速诊断测试“FalciVax”发现,13个疟疾流行地区的总体疟疾患病率为3.1%(恶性疟原虫2.73%,间日疟原虫0.16%,混合感染0.19%),在三个山区患病率最高(11%)。研究结果显示,受访者对疟疾传播、预防和治疗的了解较为肤浅。贫困和受教育程度被发现是疟疾知识和行为的重要决定因素。人们一致主张采用西医治疗,但在实际中,大多数患病者要么不寻求任何治疗(31%),要么自行治疗(12%),此时“知-行”差距尤为明显。在寻求治疗的人群中,大多数人去找乡村医生和药店销售人员(约40%)。此外,超过一半的病例在出现类似疟疾的发热症状后超过24小时才开始治疗。在调查中,观察到知识和就医行为方面存在性别差异,对女性不利。在高流行的东南部地区和低流行的东北部地区之间也存在地理差异,前者在疟疾研究的不同方面处于劣势。
本研究中的受访者缺乏关于疟疾不同方面的全面知识,这受到贫困程度和教育水平的影响。观察到知识方面存在性别和地理差异,分别对女性和东南部地区不利。他们更喜欢用西医治疗疟疾,尽管相当一部分人对类似疟疾的发热症状不寻求任何治疗或自行治疗。寻求治疗的延迟很常见。讨论了这些发现对项目开发的影响。