Department of Anesthesiology and Intensive Care, University of Rome, La Sapienza, Viale del Policlinico 155, Rome 00161, Italy.
Crit Care. 2009;13(4):R130. doi: 10.1186/cc7990. Epub 2009 Aug 10.
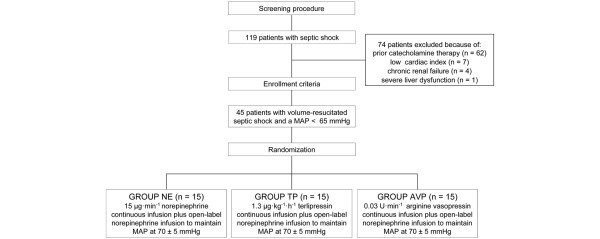
Recent clinical data suggest that early administration of vasopressin analogues may be advantageous compared to a last resort therapy. However, it is still unknown whether vasopressin and terlipressin are equally effective for hemodynamic support in septic shock. The aim of the present prospective, randomized, controlled pilot trial study was, therefore, to compare the impact of continuous infusions of either vasopressin or terlipressin, when given as first-line therapy in septic shock patients, on open-label norepinephrine requirements.
We enrolled septic shock patients (n = 45) with a mean arterial pressure below 65 mmHg despite adequate volume resuscitation. Patients were randomized to receive continuous infusions of either terlipressin (1.3 microg.kg-1.h-1), vasopressin (.03 U.min-1) or norepinephrine (15 microg.min-1; n = 15 per group). In all groups, open-label norepinephrine was added to achieve a mean arterial pressure between 65 and 75 mmHg, if necessary. Data from right heart and thermo-dye dilution catheterization, gastric tonometry, as well as laboratory variables of organ function were obtained at baseline, 12, 24, 36 and 48 hours after randomization. Differences within and between groups were analyzed using a two-way ANOVA for repeated measurements with group and time as factors. Time-independent variables were compared with one-way ANOVA.
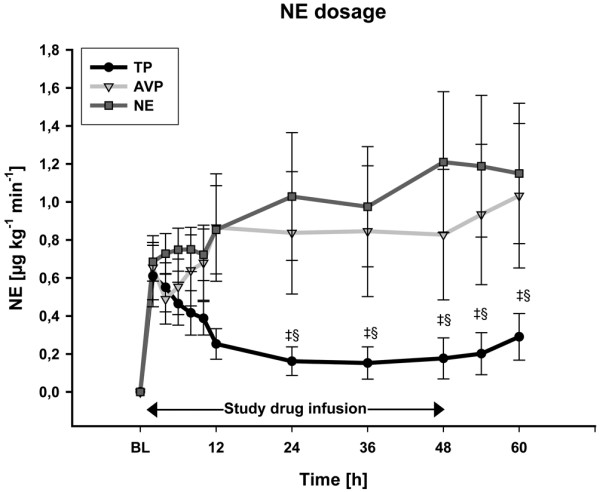
There were no differences among groups in terms of systemic and regional hemodynamics. Compared with infusion of .03 U of vasopressin or 15 microg.min-1 of norepinephrine, 1.3 microg.kg-1.h-1 of terlipressin allowed a marked reduction in catecholamine requirements (0.8 +/- 1.3 and 1.2 +/- 1.4 vs. 0.2 +/- 0.4 microg.kg-1.min-1 at 48 hours; each P < 0.05) and was associated with less rebound hypotension (P < 0.05). At the end of the 48-hour intervention period, bilirubin concentrations were higher in the vasopressin and norepinephrine groups as compared with the terlipressin group (2.3 +/- 2.8 and 2.8 +/- 2.5 vs. 0.9 +/- 0.3 mg.dL-1; each P < 0.05). A time-dependent decrease in platelet count was only observed in the terlipressin group (P < 0.001 48 hours vs. BL).
The present study provides evidence that continuous infusion of low-dose terlipressin--when given as first-line vasopressor agent in septic shock--is effective in reversing sepsis-induced arterial hypotension and in reducing norepinephrine requirements.
最近的临床数据表明,与最后手段的治疗相比,早期给予血管加压素类似物可能是有利的。然而,目前尚不清楚血管加压素和特利加压素在败血症性休克的血流动力学支持方面是否同样有效。因此,本前瞻性、随机、对照的初步试验研究的目的是比较在败血症性休克患者中作为一线治疗给予连续输注血管加压素或特利加压素对去甲肾上腺素需求的影响。
我们招募了平均动脉压低于 65 mmHg 的败血症性休克患者(n = 45),尽管进行了充分的容量复苏。患者被随机分配接受连续输注特利加压素(1.3 μg/kg-1.h-1)、血管加压素(0.03 U/min-1)或去甲肾上腺素(15 μg/min-1;每组 15 人)。在所有组中,如果需要,都将添加去甲肾上腺素以实现平均动脉压在 65 至 75 mmHg 之间。在随机分组后 12、24、36 和 48 小时,获得右心和热染料稀释导管、胃测压以及器官功能实验室变量的数据。使用双因素重复测量方差分析分析组内和组间的差异,并以组和时间为因素。使用单向方差分析比较时间独立变量。
各组在全身和局部血流动力学方面没有差异。与输注 0.03 U 血管加压素或 15 μg/min 去甲肾上腺素相比,1.3 μg/kg-1.h-1 的特利加压素可显著减少儿茶酚胺的需求(48 小时时分别为 0.8 +/- 1.3 和 1.2 +/- 1.4 与 0.2 +/- 0.4 μg/kg-1.min-1;均 P < 0.05),并与更少的反弹性低血压相关(P < 0.05)。在 48 小时干预期间,与特利加压素组相比,血管加压素和去甲肾上腺素组的胆红素浓度更高(2.3 +/- 2.8 和 2.8 +/- 2.5 与 0.9 +/- 0.3 mg/dL-1;均 P < 0.05)。仅在特利加压素组观察到血小板计数随时间的下降(P < 0.001 48 小时 vs. BL)。
本研究提供的证据表明,在败血症性休克中作为一线血管加压药给予低剂量特利加压素连续输注可有效逆转败血症引起的动脉低血压并减少去甲肾上腺素的需求。