Sefrin Peter, Brandt Michael, Kredel Markus
Klinik und Poliklinik für Anästhesiologie, Sektion für Präklinische Notfallmedizin, University of Würzburg, Germany.
Ger Med Sci. 2004 Mar 10;2:Doc02.
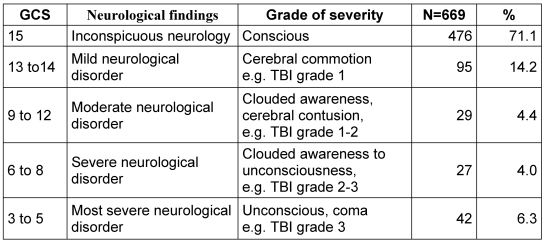
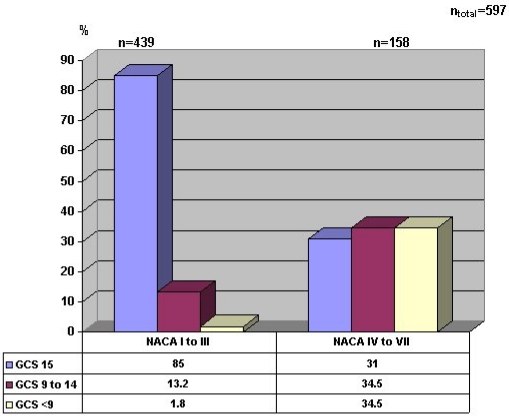
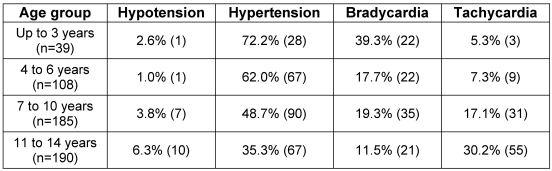
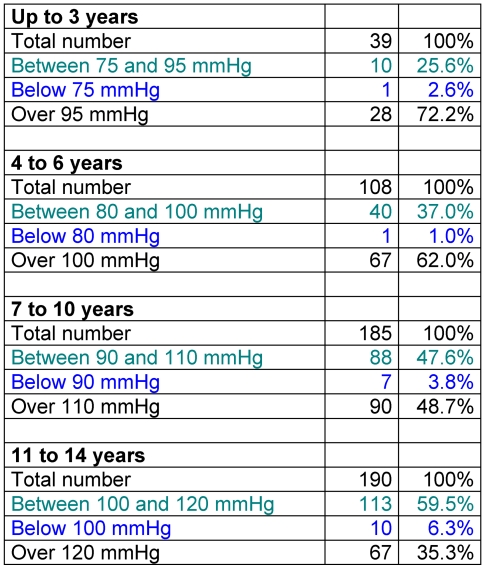
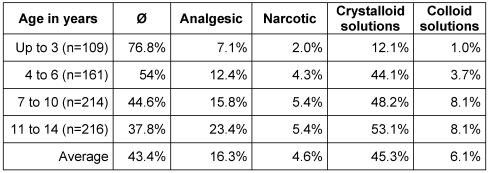
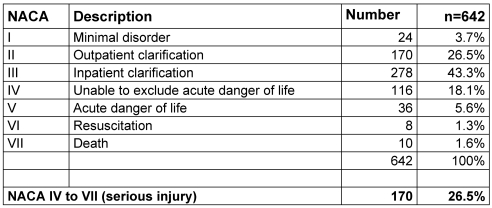
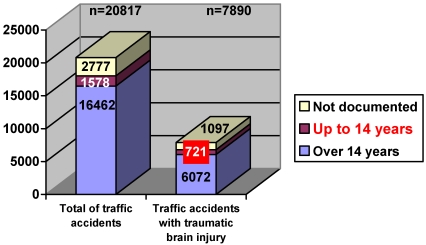
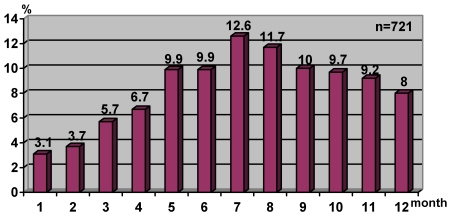
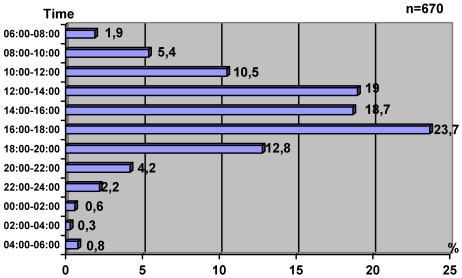
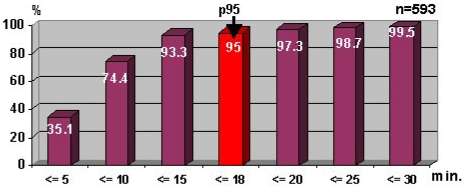
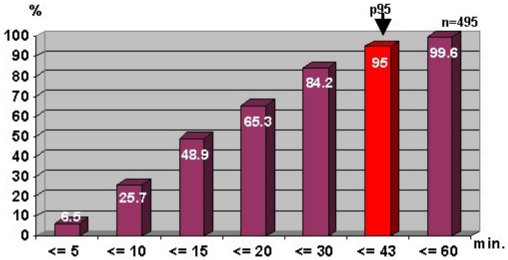
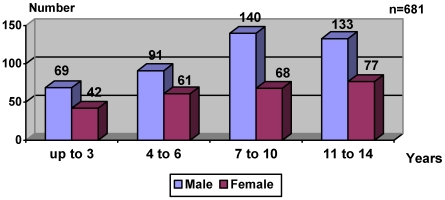
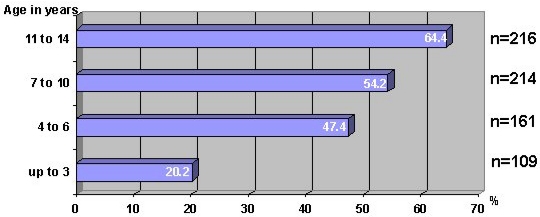
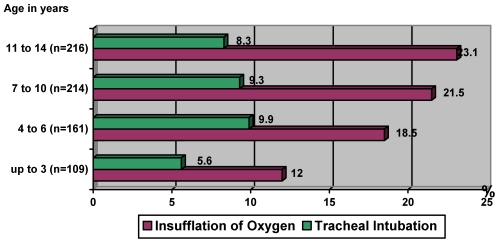
The fact that injuries caused by accidents are the most common cause of death in children and adolescents in Germany gave rise to the study, which mainly deals with traffic accidents in this group. 200,221 records of emergency-service physicians in Bavaria which cover the period 1995-1999 were analysed with respect to the importance of traumatic brain injury (TBI) in children and adolescents (n = 721 - representing 45.8% of traffic injuries in this age group). The highest incidence of TBI was in summer (34.3%) and in the evening between 16.00 and 18.00 (23.7%). The time taken between accident and arrival of the emergency services was 8.8 +/- 3.1 minutes. The preclinical phase lasted 19.3 +/- 5.8 minutes. The probability of having an accident with TBI increases with age, the maximum being in the age-range 7 - 14 years (61.6%). Boys (63.2%) were almost twice as susceptible to injury as girls. 36.8% of all cases had no noticeable neurological disorder, 71.1% resulted in a Glasgow Coma Scale (GCS) score of 15. Only 6.3% had most severe neurological disorders, resulting in a GCS score of 3 - 5. Circulation parameters in the form of adapted hypotension were abnormal in only 3.4%, 21.9% of the children had a bradycardia and in 12.3% the blood oxygen saturation fell below 94%. The most frequent intervention was the laying of an i.v. line for infusions. 8.6% of the patients were intubated to allow for ventilation with oxygen. Analgesics were given in 16.7% of the cases. In 84.7% of all cases, the condition was stable and in only 3.3% was a severe deterioration to be observed. The assessments were made using both the National Advisory Committee for Aeronautics (NACA) and Glasgow Coma Scales (GCS). Discrepancies occurred, as a NACA scale of I - III and a GCS score of < 9 was reported in 4.9% of cases. In contrast a NACA scale of IV - VI was reported with a GCS score of 15 in 30% of all cases. TBI symptoms in children are less obvious than in adults, which leads to an age-dependent restriction in implementing therapeutic measures. If these restrictions are a result of misinterpretation of the situation or due to a lack of practice in the preclinical phase, then further training and education of the physicians involved in emergency service work are necessary.
在德国,事故造成的伤害是儿童和青少年最常见的死亡原因,这一事实引发了这项主要针对该群体交通事故的研究。分析了巴伐利亚州急救医生在1995 - 1999年期间的200,221份记录,以了解创伤性脑损伤(TBI)在儿童和青少年中的重要性(n = 721,占该年龄组交通伤的45.8%)。TBI的最高发病率出现在夏季(34.3%)以及傍晚16:00至18:00之间(23.7%)。事故发生到急救服务到达的时间为8.8 +/- 3.1分钟。临床前阶段持续19.3 +/- 5.8分钟。发生伴有TBI事故的概率随年龄增加,在7 - 14岁年龄组达到最高(61.6%)。男孩(63.2%)受伤的易感性几乎是女孩的两倍。所有病例中36.8%没有明显的神经功能障碍,71.1%的病例格拉斯哥昏迷量表(GCS)评分为15分。只有6.3%的病例有最严重的神经功能障碍,GCS评分为3 - 5分。以适应性低血压形式出现的循环参数异常仅占3.4%,21.9%的儿童有心动过缓,12.3%的儿童血氧饱和度低于94%。最常见的干预措施是静脉置管输液。8.6%的患者进行了气管插管以便吸氧通气。16.7%的病例使用了镇痛药。在所有病例中,84.7%的病情稳定,只有3.3%观察到病情严重恶化。评估使用了美国国家航空咨询委员会(NACA)量表和格拉斯哥昏迷量表(GCS)。出现了差异,4.9%的病例报告NACA量表为I - III级且GCS评分<9分。相比之下,30%的病例报告NACA量表为IV - VI级且GCS评分为15分。儿童的TBI症状不如成人明显,这导致在实施治疗措施时存在年龄依赖性限制。如果这些限制是由于对情况的误解或临床前阶段缺乏实践造成的,那么有必要对参与急救服务工作的医生进行进一步培训和教育。