Schwille Paul O, Schmiedl A, Wipplinger J
Mineral Metabolism and Endocrine Research Laboratory, Departments of Surgery and Urology, University of Erlangen-Nürnberg, Germany.
Eur J Med Res. 2009 Sep 1;14(9):378-92. doi: 10.1186/2047-783x-14-9-378.
In IRCU it is uncertain whether variation of urinary protein, especially non-albumin protein (N-Alb-P), is due to the presence of stones or reflects alteration of oxidative metabolism.
To validate in a tripartite cross-sectional study of 187 ambulatory male patients, undergoing a standardized laboratory programme, whether stones impact on N-Alb-P or the state of oxidative metabolism interferes with IRCU pathophysiology.
In part 1 the strata low and high of fasting urinary excretion rate per 2 h of N-Alb-P, malonedialdehyde, hypoxanthine, xanthine, pH and other urine components were compared, and association with renal stones in situ evaluated; in part 2 the co-variation of oxidatively modulated environment, fasting urinary pH, calcium (Ca) salt crystallization risk and the number of patients with stones in situ was examined; in part 3, the nucleation of Ca oxalate and Ca phosphate was tested in undiluted postprandial urine of patients and related to the state of oxidative metabolism.
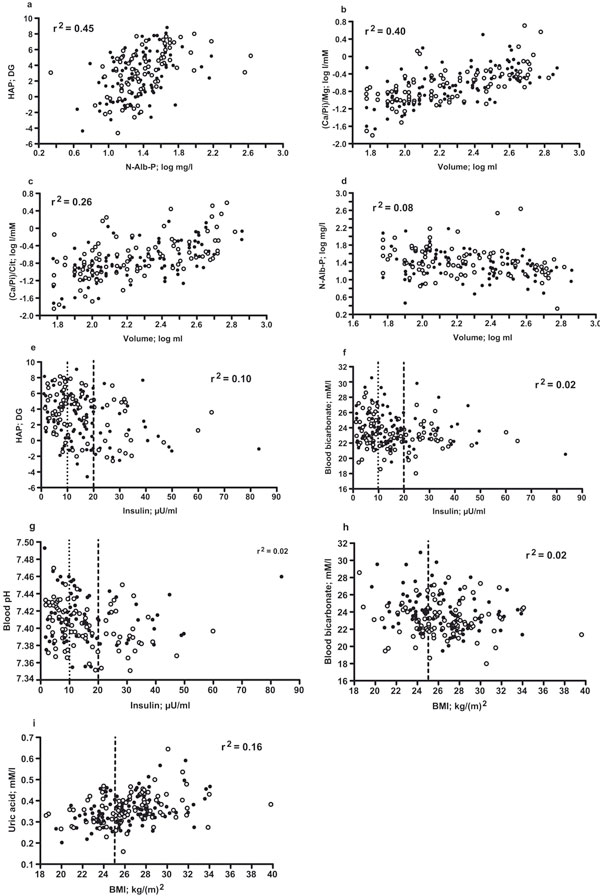
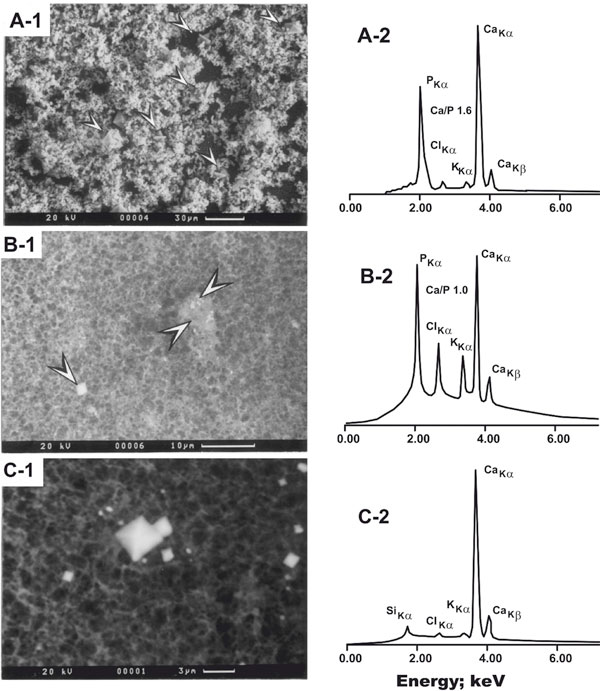
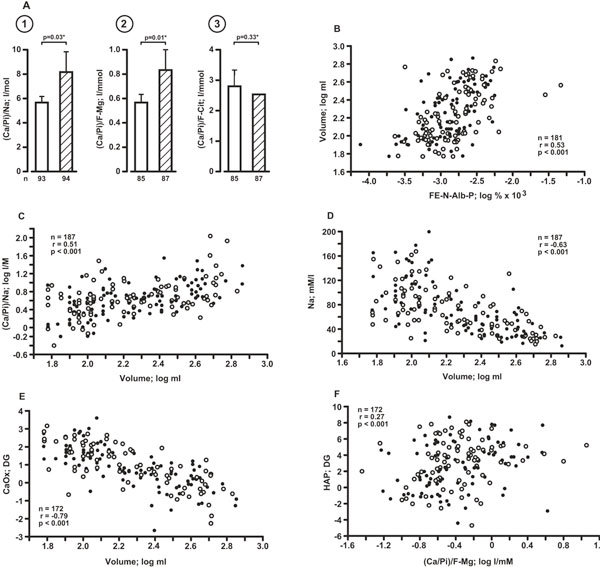
In part 1, N-Alb-P excretion >4.3 mg was associated with increase of blood pressure, excretion of total protein, hypoxanthine (a marker of tissue hypoxia), malonedialdehyde (a marker of lipid peroxidation), sodium, magnesium, citrate, uric acid, volume, pH, and increase of renal fractional excretion of both N-Alb-P and uric acid; when stones were present, urinary pH was elevated but other parameters were unaffected. Significant predictors of N-Alb-P excretion were malonedialdehyde, fractional N-Alb-P and hypoxanthine. In part 2, urine pH >6.14 was associated with unchanged blood pressure and plasma vasopressin, increase of blood pH, urinary volume, malonedialdehyde, fractional excretion of N-Alb-P, uric acid, Ca phosphate, but not Ca oxalate, supersaturation; this spectrum was accompanied by decrease of concentration of urinary total and free magnesium, total and complexed citrate, plasma uric acid (in humans the major circulating antioxidant) and insulin; the number of stone-bearing patients was increased. Significant predictors of urine pH were body mass index, plasma insulin and uric acid (negative), and urinary xanthine (positive). In part 3 low plasma uric acid, not high urinary malonedialdehyde or high ratio malonedialdehyde/uric acid was significantly associated with diminished Ca but not oxalate tolerance, with the first nucleating crystal type being mostly Ca phosphate (hydroxyapatite), in the rest Ca oxalate dihydrate; uricemia correlated marginally positively (p = 0.055) with Ca tolerance of urine, stronger with blood pressure and insulin, and negatively with urinary xanthine, fractional N-Alb-P, volume, sodium.
In IRCU 1) not renal stones in situ, but disturbed oxidative metabolism apparently modulates nephron functionality, ending up in higher renal N-Alb-P release, urinary volume, sodium and pH of fasting urine; 2) etiologically unknown decline of uricemia may represent antioxidant deficiency and cause a risk of hydroxyapatite crystallization and stone formation in a weakly acidic or alkaline inhibitor-deficient and N-Alb-P-rich milieu; 3) several observations, linking oxidative and systemic metabolism, are compatible with Ca stone initiation beyond tubules.
在特发性肾小管间质性肾炎(IRCU)中,尿蛋白尤其是非白蛋白蛋白(N-Alb-P)的变化是由于结石的存在,还是反映氧化代谢的改变尚不确定。
在一项对187名接受标准化实验室检查的门诊男性患者进行的三方横断面研究中,验证结石是否会影响N-Alb-P,或者氧化代谢状态是否会干扰IRCU的病理生理过程。
在第一部分中,比较了每2小时N-Alb-P、丙二醛、次黄嘌呤、黄嘌呤、pH值和其他尿液成分的空腹尿排泄率的高低分层,并评估与原位肾结石的相关性;在第二部分中,检查了氧化调节环境、空腹尿pH值、钙(Ca)盐结晶风险和原位结石患者数量的协变量;在第三部分中,在患者的餐后未稀释尿液中测试草酸钙和磷酸钙的成核情况,并与氧化代谢状态相关联。
在第一部分中,N-Alb-P排泄>4.3mg与血压升高、总蛋白排泄、次黄嘌呤(组织缺氧标志物)、丙二醛(脂质过氧化标志物)、钠、镁、柠檬酸盐、尿酸、尿量、pH值升高以及N-Alb-P和尿酸的肾分数排泄增加有关;当存在结石时,尿pH值升高,但其他参数未受影响。N-Alb-P排泄的显著预测因素是丙二醛、N-Alb-P分数和次黄嘌呤。在第二部分中,尿pH>6.14与血压和血浆血管加压素不变、血液pH值、尿量、丙二醛、N-Alb-P分数排泄、尿酸、磷酸钙(而非草酸钙)过饱和度增加有关;这一系列变化伴随着尿总镁和游离镁、总柠檬酸盐和络合柠檬酸盐、血浆尿酸(人类主要循环抗氧化剂)和胰岛素浓度的降低;结石患者数量增加。尿pH值的显著预测因素是体重指数、血浆胰岛素和尿酸(负相关)以及尿黄嘌呤(正相关)。在第三部分中,低血浆尿酸,而非高尿丙二醛或高丙二醛/尿酸比值,与钙耐受性降低显著相关,但与草酸盐耐受性无关,第一种成核晶体类型主要是磷酸钙(羟基磷灰石),其余为二水合草酸钙;血尿酸与尿钙耐受性呈微弱正相关(p = 0.055),与血压和胰岛素的相关性更强,与尿黄嘌呤、N-Alb-P分数、尿量、钠呈负相关。
在IRCU中,1)不是原位肾结石,而是氧化代谢紊乱明显调节肾单位功能,最终导致肾N-Alb-P释放增加、尿量、钠和空腹尿pH值升高;2)病因不明的血尿酸下降可能代表抗氧化剂缺乏,并在弱酸性或碱性抑制剂缺乏且N-Alb-P丰富的环境中导致羟基磷灰石结晶和结石形成的风险;3)一些将氧化代谢与全身代谢联系起来的观察结果与肾小管外的钙结石形成相符。