McGill University AIDS Centre, Jewish General Hospital, Montreal, Quebec, Canada.
J Int AIDS Soc. 2009 Oct 25;12:25. doi: 10.1186/1758-2652-12-25.
Our objective was to establish genotypic resistance profiles among the 4% of Batswana patients who experienced virologic failure while being followed within Botswana's National Antiretroviral Treatment Program between 2002 and 2007.
At the beginning of the national program in 2002, almost all patients received stavudine (d4T), together with didanosine (ddI), as part of their first nucleoside reverse transcriptase inhibitor (NRTI)-based regimen (Group 1). In contrast, the standard of care for all patients subsequently enrolled (2002-2007) included zidovudine/lamivudine (ZDV/3TC) (Group 2). Genotypes were analyzed in 26 patients from Group 1 and 37 patients from Group 2. Associations between mutations were determined using Pearson's correlation coefficient and Jaccard's coefficient of similarity.
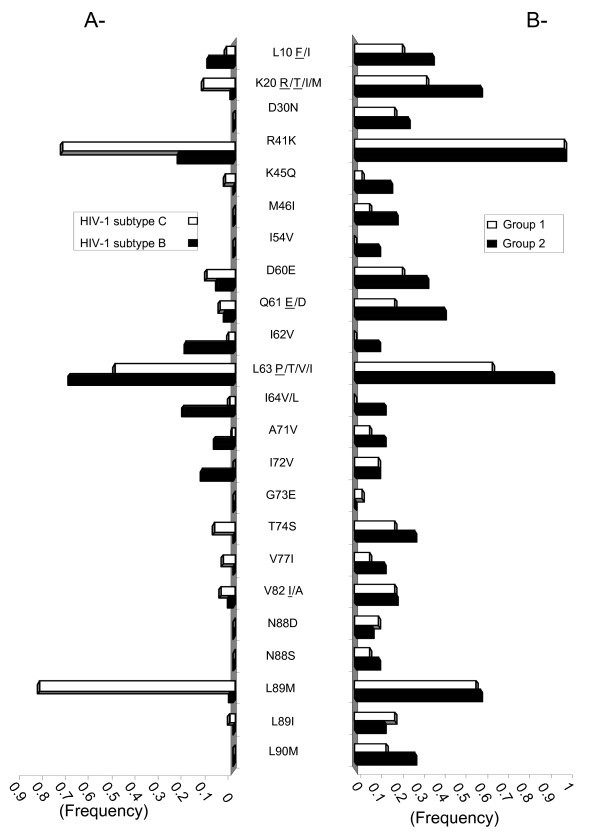
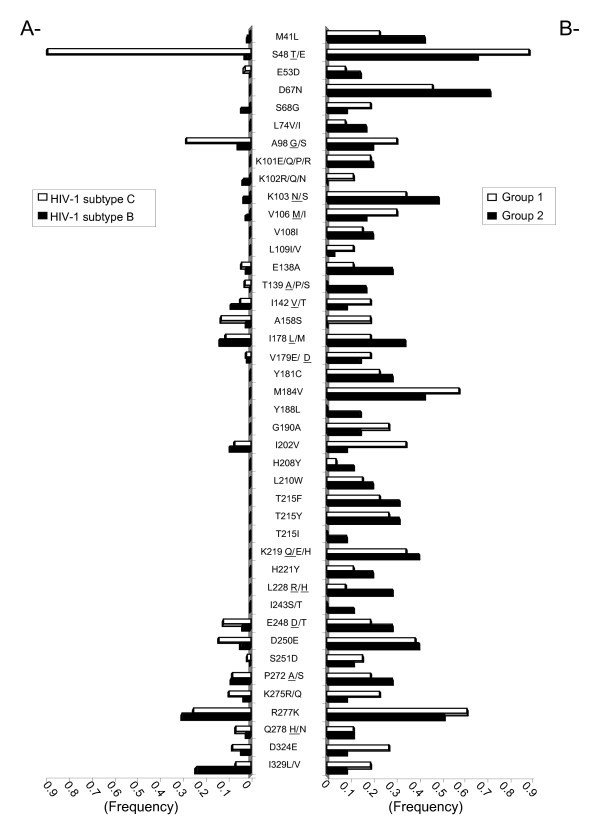
Seventy-eight percent of genotyped patients possessed mutations associated with protease inhibitor (PI) resistance while 87% and 90%, respectively, exhibited mutations associated with NRTIs and non-nucleoside reverse transcriptase inhibitors (NNRTIs). The most frequent PI mutations involving resistance to NFV were L90M (25.2%) and D30N (16.2%), but mutations at positions K45Q and D30N were often observed in tandem (P = 60.5, J = 50; p = 0.002; Group 2) alongside Q61E in 42.8% of patients who received ZDV/3TC. Both major patterns of thymidine analogue mutations, TAM 1 (48%) and TAM 2 (59%), were represented in patients from Group 1 and 2, although M184V was higher among individuals who had initially received ddI (61% versus 40.5%). In contrast, L74V was more frequent among individuals from Group 2 (16.2% versus 7.7%). Differences in regard to NNRTI mutations were also observed between Group 1 and Group 2 patients.
Despite a low rate of therapeutic failure (4%) among these patients, those who failed possessed high numbers of resistance mutations as well as novel resistance mutations and/or polymorphisms at sites within reverse transcriptase and protease.
在 2002 年至 2007 年期间,博茨瓦纳国家抗逆转录病毒治疗计划对 4%发生病毒学失败的患者进行随访,本研究旨在建立这些患者的基因型耐药谱。
2002 年国家项目启动之初,几乎所有患者都接受了司他夫定(d4T)加去羟肌苷(ddI)治疗,作为他们的首个基于核苷逆转录酶抑制剂(NRTI)的方案的一部分(第 1 组)。相比之下,所有随后入组的患者(2002-2007 年)均接受齐多夫定/拉米夫定(ZDV/3TC)治疗(第 2 组)。对第 1 组的 26 名患者和第 2 组的 37 名患者进行了基因型分析。采用 Pearson 相关系数和 Jaccard 相似系数来确定突变之间的相关性。
78%的基因分型患者存在与蛋白酶抑制剂(PI)耐药相关的突变,而分别有 87%和 90%的患者存在与 NRTIs 和非核苷逆转录酶抑制剂(NNRTIs)耐药相关的突变。涉及 NFV 耐药的最常见 PI 突变包括 L90M(25.2%)和 D30N(16.2%),但 K45Q 和 D30N 位置的突变常常同时出现(P=60.5,J=50;p=0.002;第 2 组),同时在接受 ZDV/3TC 治疗的患者中,42.8%的患者出现 Q61E 突变。第 1 组和第 2 组患者均存在主要的胸苷类似物突变模式,TAM1(48%)和 TAM2(59%),但在最初接受 ddI 治疗的患者中,M184V 更为常见(61%对 40.5%)。相反,L74V 在第 2 组患者中更为常见(16.2%对 7.7%)。第 1 组和第 2 组患者的 NNRTI 突变也存在差异。
尽管这些患者的治疗失败率(4%)较低,但失败的患者存在大量耐药突变以及逆转录酶和蛋白酶内新的耐药突变和/或多态性。