Department of Anaesthesiology and Intensive Care Medicine, University Hospital Schleswig-Holstein, Kiel, Germany.
PLoS One. 2009 Oct 26;4(10):e7588. doi: 10.1371/journal.pone.0007588.
Mild therapeutic hypothermia following cardiac arrest is neuroprotective, but its effect on myocardial dysfunction that is a critical issue following resuscitation is not clear. This study sought to examine whether hypothermia and the combination of hypothermia and pharmacological postconditioning are cardioprotective in a model of cardiopulmonary resuscitation following acute myocardial ischemia.
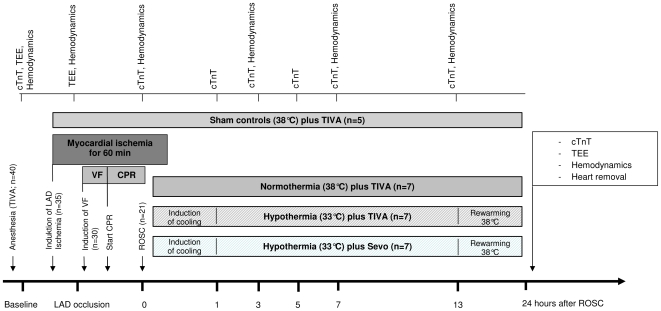
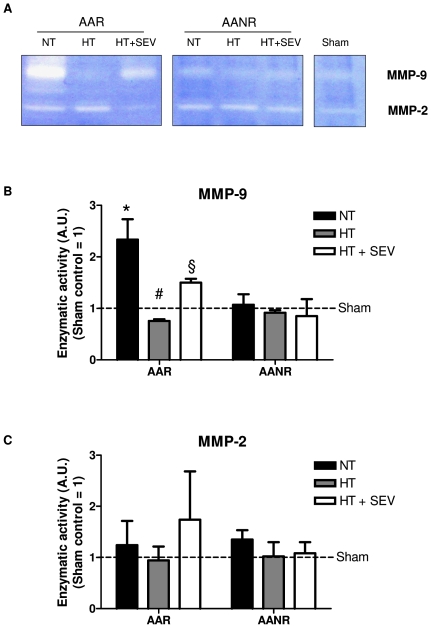
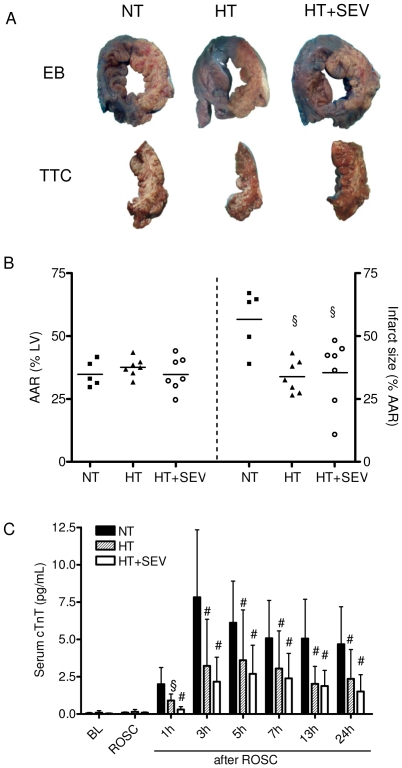
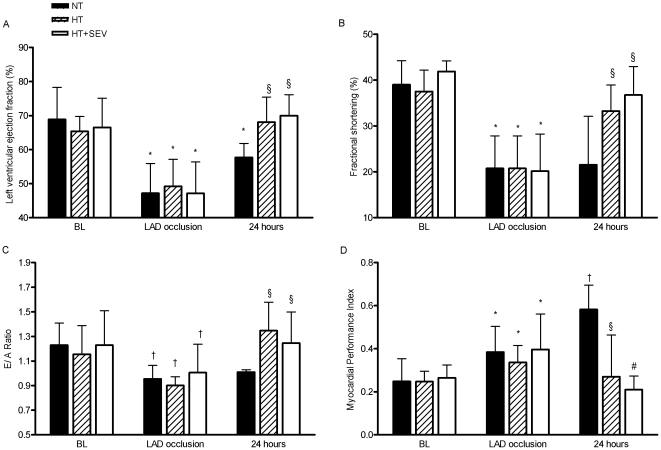
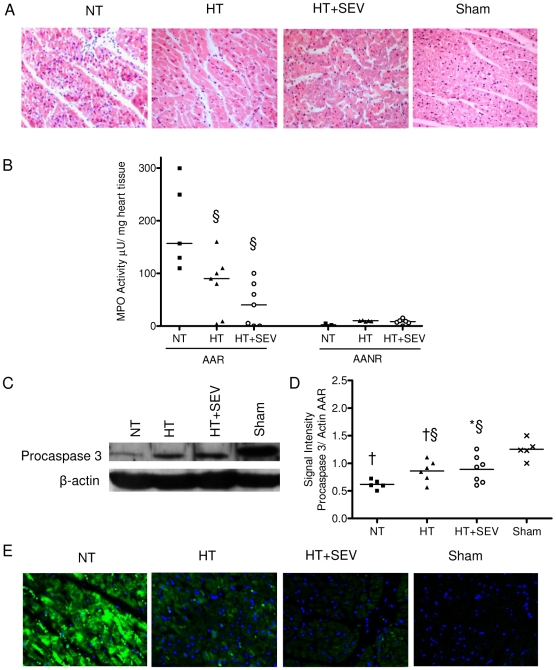
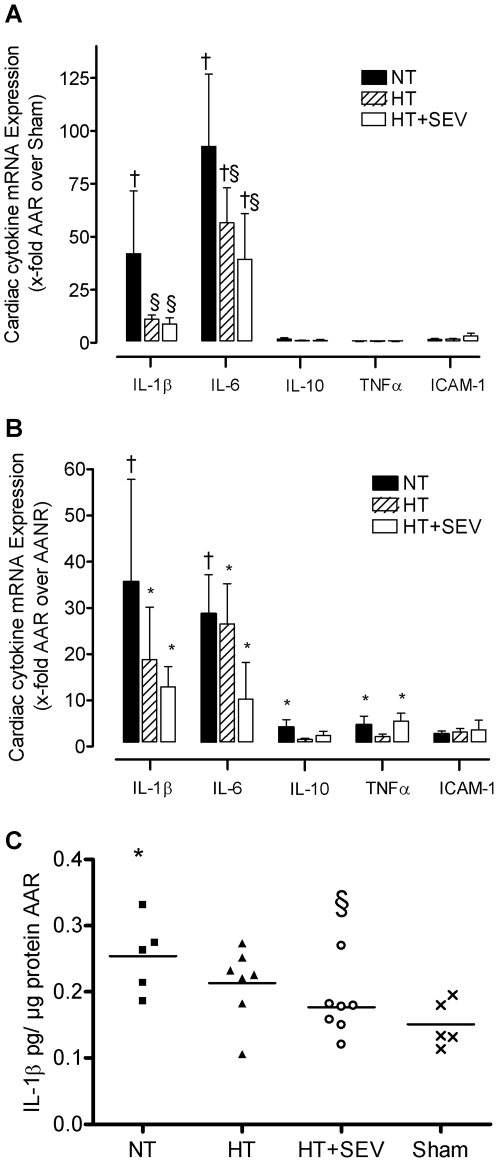
METHODOLOGY/PRINCIPAL FINDINGS: Thirty pigs (28-34 kg) were subjected to cardiac arrest following left anterior descending coronary artery ischemia. After 7 minutes of ventricular fibrillation and 2 minutes of basic life support, advanced cardiac life support was started according to the current AHA guidelines. After successful return of spontaneous circulation (n = 21), coronary perfusion was reestablished after 60 minutes of occlusion, and animals were randomized to either normothermia at 38 degrees C, hypothermia at 33 degrees C or hypothermia at 33 degrees C combined with sevoflurane (each group n = 7) for 24 hours. The effects on cardiac damage especially on inflammation, apoptosis, and remodeling were studied using cellular and molecular approaches. Five animals were sham operated. Animals treated with hypothermia had lower troponin T levels (p<0.01), reduced infarct size (34+/-7 versus 57+/-12%; p<0.05) and improved left ventricular function compared to normothermia (p<0.05). Hypothermia was associated with a reduction in: (i) immune cell infiltration, (ii) apoptosis, (iii) IL-1beta and IL-6 mRNA up-regulation, and (iv) IL-1beta protein expression (p<0.05). Moreover, decreased matrix metalloproteinase-9 activity was detected in the ischemic myocardium after treatment with mild hypothermia. Sevoflurane conferred additional protective effects although statistic significance was not reached.
CONCLUSIONS/SIGNIFICANCE: Hypothermia reduced myocardial damage and dysfunction after cardiopulmonary resuscitation possible via a reduced rate of apoptosis and pro-inflammatory cytokine expression.
心脏骤停后进行轻度治疗性低温对神经有保护作用,但对于复苏后心肌功能障碍这一关键问题的影响尚不清楚。本研究旨在探讨心肺复苏后急性心肌缺血模型中,低温和低温联合药物后处理是否具有心肌保护作用。
方法/主要发现:30 头(28-34 公斤)猪经历左前降支冠状动脉缺血后发生心脏骤停。室颤 7 分钟和基础生命支持 2 分钟后,根据当前 AHA 指南开始进行高级心脏生命支持。自主循环恢复成功后(n=21),闭塞 60 分钟后再灌注冠状动脉,并将动物随机分为常温 38°C 组、低温 33°C 组或低温 33°C 联合七氟醚(每组 n=7)24 小时。使用细胞和分子方法研究心脏损伤,特别是炎症、细胞凋亡和重构的影响。5 头动物作为假手术组。与常温组相比,低温组肌钙蛋白 T 水平较低(p<0.01),梗死面积较小(34+/-7 比 57+/-12%;p<0.05),左心室功能改善(p<0.05)。低温治疗与以下因素减少有关:(i)免疫细胞浸润,(ii)细胞凋亡,(iii)IL-1beta 和 IL-6 mRNA 上调,和(iv)IL-1beta 蛋白表达(p<0.05)。此外,在轻度低温治疗后,缺血心肌中检测到基质金属蛋白酶-9 活性降低。七氟醚联合治疗有额外的保护作用,尽管未达到统计学意义。
结论/意义:低温可通过降低细胞凋亡和促炎细胞因子表达来减少心肺复苏后心肌损伤和功能障碍。