Department of Anesthesiology, Baylor College of Medicine, Division of Pediatric Cardiovascular Anesthesiology, Texas Children's Hospital, 6621 Fannin, WT 17417B, Houston, TX 77030, USA.
J Thorac Cardiovasc Surg. 2010 Mar;139(3):543-56. doi: 10.1016/j.jtcvs.2009.08.022. Epub 2009 Nov 11.
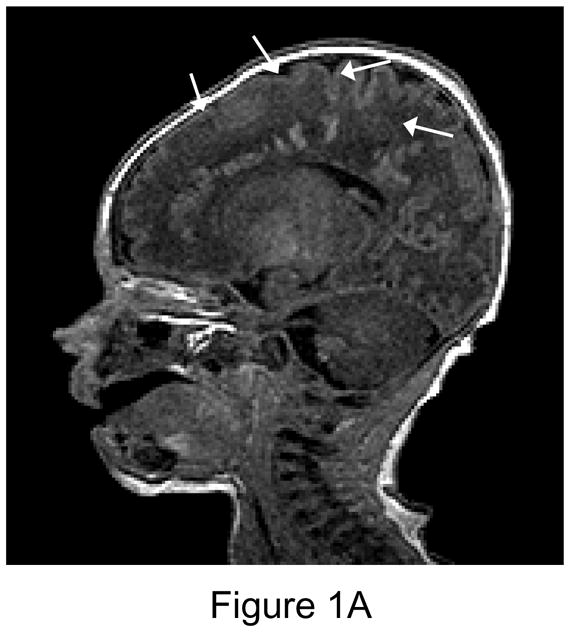
New intraparenchymal brain injury on magnetic resonance imaging is observed in 36% to 73% of neonates after cardiac surgery with cardiopulmonary bypass. Brain immaturity in this population is common. We performed brain magnetic resonance imaging before and after neonatal cardiac surgery, using a high-flow cardiopulmonary bypass protocol, hypothesizing that brain injury on magnetic resonance imaging would be associated with brain immaturity.
Cardiopulmonary bypass protocol included 150 mL . kg(-1) . min(-1) flows, pH stat management, hematocrit > 30%, and high-flow antegrade cerebral perfusion. Regional brain oxygen saturation was monitored, with a treatment protocol for regional brain oxygen saturation < 50%. Brain magnetic resonance imaging, consisting of T1-, T2-, and diffusion-weighted imaging, and magnetic resonance spectroscopy were performed preoperatively, 7 days postoperatively, and at age 3 to 6 months.
Twenty-four of 67 patients (36%) had new postoperative white matter injury, infarction, or hemorrhage, and 16% had new white matter injury. Associations with preoperative brain injury included low brain maturity score (P = .002). Postoperative white matter injury was associated with single-ventricle diagnosis (P = .02), preoperative white matter injury (P < .001), and low brain maturity score (P = .05). Low brain maturity score was also associated with more severe postoperative brain injury (P = .01). Forty-five patients had a third scan, with a 27% incidence of new minor lesions, but 58% of previous lesions had partially or completely resolved.
We observed a significant incidence of both pre- and postoperative magnetic resonance imaging abnormality and an association with brain immaturity. Many lesions resolved in the first 6 months after surgery. Timing of delivery and surgery with bypass could affect the risk of brain injury.
在体外循环心脏手术后,36%至 73%的新生儿在磁共振成像上观察到新的脑内损伤。该人群的脑不成熟很常见。我们在新生儿心脏手术后使用高流量体外循环方案进行了脑磁共振成像,假设磁共振成像上的脑损伤与脑不成熟有关。
体外循环方案包括 150 毫升/千克/分钟的流量、pH -stat 管理、血细胞比容>30%和高流量顺行脑灌注。监测区域性脑氧饱和度,制定区域性脑氧饱和度<50%的治疗方案。磁共振成像包括 T1、T2 和弥散加权成像以及磁共振波谱,在术前、术后 7 天和 3 至 6 个月龄进行。
24 例(36%)患者在术后出现新的脑白质损伤、梗死或出血,16%患者出现新的脑白质损伤。与术前脑损伤相关的因素包括脑成熟评分低(P=0.002)。术后脑白质损伤与单心室诊断(P=0.02)、术前脑白质损伤(P<0.001)和脑成熟评分低(P=0.05)相关。脑成熟评分低也与术后更严重的脑损伤相关(P=0.01)。45 例患者进行了第三次扫描,新出现轻微病变的发生率为 27%,但 58%的既往病变已部分或完全消退。
我们观察到磁共振成像异常的发生率很高,包括术前和术后,并与脑不成熟有关。许多病变在手术后的头 6 个月内得到缓解。分娩时间和手术与体外循环的时间间隔可能会影响脑损伤的风险。