Neto Arnaldo Moura, Tambascia Marcos Antonio, Brunetto Sergio, Ramos Celso Dario, Zantut-Wittmann Denise Engelbrecht
Endocrinology Division, Internal Medicine Department, Medical Science School, University of Campinas, Campinas, S.P., Brazil.
Cases J. 2009 Aug 25;2:8479. doi: 10.4076/1757-1626-2-8479.
Radioactive iodine ((131)I) is widely prescribed for treatment of Graves' disease. A dose of 370 to 555 MBq (10 to 15 mCi) is usually enough, but reports of improved remission rates with single doses up to 20-30 mCi, and 38.5 mCi at most, exist.
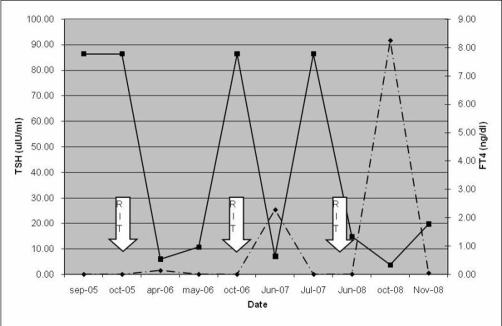
A 53-year-old male patient was evaluated in September 2005, with symptoms of thyrotoxicosis for 2 years. He presented with tachycardia (130 bpm) and a large goiter. Thyrotropin was <0.01 uIU/ml (0,41-4,5), free thyroxin >7.77 ng/dl (0.9-1.8), anti-thyreoperoxidase antibody: 374 IU/ml (<35) and anti-thyroglobulin antibody: 749 IU/ml (<115). Ultrasound: diffuse goiter, no nodules; right lobe: 7.9 x 3.8 x 3.8 cm; left: 7.7 x 3.5 x 3.8 cm; isthmus: 1.6 cm. Propylthiouracil 300 mg t.i.d. and propranolol were prescribed. Thyroid (99m)Tc-pertechnetate uptake: 52% (0.35-1.7%) and estimated thyroid volume: 149 mL. After 30 days, he received 555 MBq (15 mCi) of (131)I-iodide. Six months after radioiodine therapy, under methimazole 40 mg, thyroid stimulating hormone was 1.5 uIU/ml; free thyroxine 0.54 ng/dl. Methimazole was suspended. In 21 days, thyroid stimulating hormone was 0.03 uIU/ml; free thyroxine 0.96 ng/dl. Methimazole was reintroduced. One year later, thyroid stimulating hormone was <0.01 uIU/ml and free thyroxine >7.77 ng/dl. Thyroid (99m)Tc-pertechnetate uptake was 45% and estimated thyroid volume 144 mL. A 1110 MBq (30 mCi) radioiodine therpy was administered. He used Methimazole for 8 months, when overt hypothyroidism appeared (TSH: 25.30 uIU/ml; free thyroxine: 0.64 ng/dl). Methimazole was interrupted. Hyperthyroidism returned 6 weeks later (thyroid stimulating hormone <0.01 uIU/ml; free thyroxine >7.77 ng/dl). Thyroid (99m)Tc-pertechnetate uptake was 25% and estimated thyroid volume 111 mL. Methimazole was prescribed again. In March 2008 he received a 2590 MBq (70 mCi) radioiodine therapy. By may/2008, under methimazole 20 mg, his TSH was 0.07 uIU/ml; free thyroxine 1.31 ng/dl. In October 2008 he presented overt hypothyroidism (TSH 91.6 uIU/ml; free thyroxine 0.34) and was given levothyroxine 75 mcg/day. He remains euthyroid under hormone replacement.
Our presented case of Graves' disease received a cumulative dose of 4255 MBq (115 mCi). The high uptake could indicate accelerated iodine turnover with (131)I short time of action. Impaired hormone synthesis could also be present. We believe the extremely high dose required was due to the initial very high iodine uptake and large thyroid volume.
放射性碘(¹³¹I)被广泛用于治疗格雷夫斯病。通常370至555兆贝可(10至15毫居里)的剂量就足够了,但也有报告称单剂量高达20 - 30毫居里,最多38.5毫居里时缓解率有所提高。
一名53岁男性患者于2005年9月接受评估,有甲状腺毒症症状2年。他表现为心动过速(130次/分钟)和巨大甲状腺肿。促甲状腺激素<0.01微国际单位/毫升(0.41 - 4.5),游离甲状腺素>7.77纳克/分升(0.9 - 1.8),抗甲状腺过氧化物酶抗体:374国际单位/毫升(<35),抗甲状腺球蛋白抗体:749国际单位/毫升(<115)。超声检查:弥漫性甲状腺肿,无结节;右叶:7.9×3.8×3.8厘米;左叶:7.7×3.5×3.8厘米;峡部:1.6厘米。给予丙硫氧嘧啶300毫克,每日三次及普萘洛尔。甲状腺(⁹⁹ᵐTc)高锝酸盐摄取率:52%(0.35 - 1.7%),估计甲状腺体积:149毫升。30天后,他接受了555兆贝可(15毫居里)的¹³¹I - 碘化物治疗。放射性碘治疗6个月后,在服用甲巯咪唑40毫克的情况下,促甲状腺激素为1.5微国际单位/毫升;游离甲状腺素0.54纳克/分升。停用甲巯咪唑。21天后,促甲状腺激素为0.03微国际单位/毫升;游离甲状腺素0.96纳克/分升。重新使用甲巯咪唑。一年后,促甲状腺激素<0.01微国际单位/毫升,游离甲状腺素>7.77纳克/分升。甲状腺(⁹⁹ᵐTc)高锝酸盐摄取率为45%,估计甲状腺体积144毫升。给予1110兆贝可(30毫居里)放射性碘治疗。他服用甲巯咪唑8个月后出现明显甲状腺功能减退(促甲状腺激素:25.30微国际单位/毫升;游离甲状腺素:0.64纳克/分升)。停用甲巯咪唑。6周后甲亢复发(促甲状腺激素<0.01微国际单位/毫升;游离甲状腺素>7.77纳克/分升)。甲状腺(⁹⁹ᵐTc)高锝酸盐摄取率为25%,估计甲状腺体积111毫升。再次给予甲巯咪唑。2008年3月他接受了2590兆贝可(70毫居里)放射性碘治疗。到2008年5月,在服用甲巯咪唑20毫克的情况下,他的促甲状腺激素为0.07微国际单位/毫升;游离甲状腺素1.31纳克/分升。2008年10月他出现明显甲状腺功能减退(促甲状腺激素91.6微国际单位/毫升;游离甲状腺素0.34),并给予左甲状腺素75微克/天。他在激素替代治疗下保持甲状腺功能正常。
我们所呈现的格雷夫斯病病例接受的累积剂量为4255兆贝可(115毫居里)。高摄取可能表明¹³¹I作用时间短导致碘周转加速。也可能存在激素合成受损。我们认为所需的极高剂量是由于最初的碘摄取非常高以及甲状腺体积大。