Department of GI Surgery, Medway Maritime Hospital, King's College, UK.
World J Emerg Surg. 2009 Nov 30;4:44. doi: 10.1186/1749-7922-4-44.
Femoral hernias are relatively uncommon, however they are the most common incarcerated abdominal hernia, with strangulation of a viscus carrying significant mortality. Classically three approaches are described to open femoral hernia repair: Lockwood's infra-inguinal, Lotheissen's trans-inguinal and McEvedy's high approach. Each approach describes a separate skin incision and dissection to access the femoral sac. The decision as to which approach to adopt, predominantly dependent on the suspicion of finding strangulated bowel, is often a difficult one and in our opinion an unnecessary one.
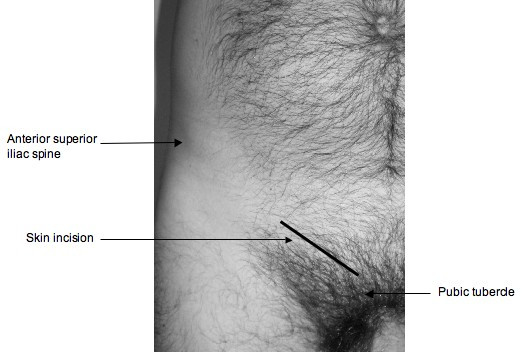
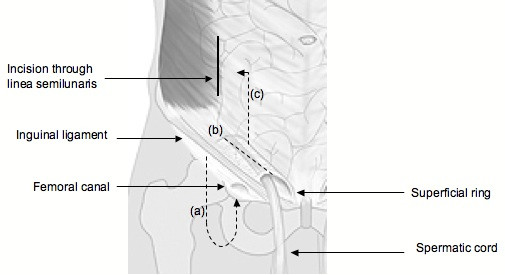
We propose a technique for open femoral hernia repair that involves a single skin incision 1 cm above the medial half of the inguinal ligament that allows all of the above approaches to the hernia sac depending on the operative findings. Thus the repair of simple femoral hernias can be performed from below the inguinal ligament. If found, inguinal hernias can be repaired. More importantly, resection of compromised bowel can be achieved by accessing the peritoneal cavity with division of the linea semilunaris 4 cm above the inguinal ligament. This avoids compromise of the inguinal canal, and with medial retraction of the rectus abdominis muscle enables access to the peritoneal cavity and compromised bowel.
This simple technique minimises the preoperative debate as to which incision will allow the best approach to the femoral hernia sac, allow for alteration to a simple inguinal hernia repair if necessary, and more importantly obviate the need for further skin incisions if compromised bowel is encountered that requires resection.
股疝相对少见,但它们是最常见的嵌顿性腹部疝,伴发内脏绞窄的死亡率较高。经典的股疝修补术有三种入路方式:Lockwood 的腹股沟下、Lotheissen 的经腹股沟和 McEvedy 的高位入路。每种入路方式都描述了一个单独的皮肤切口和解剖来进入股疝囊。选择采用哪种入路方式,主要取决于是否怀疑有绞窄性肠管,这通常是一个困难的决定,我们认为这是不必要的。
我们提出了一种开放股疝修补术的技术,该技术涉及在腹股沟韧带内侧半上方 1 厘米处的单个皮肤切口,根据手术发现,可以采用上述所有方法进入疝囊。因此,简单股疝的修补可以在腹股沟韧带下方进行。如果发现腹股沟疝,可以进行修补。更重要的是,可以通过在腹股沟韧带上方 4 厘米处切开半月线进入腹腔,切除受损的肠管。这样可以避免腹股沟管受损,通过腹直肌的内侧牵引,可以进入腹腔和受损的肠管。
这种简单的技术最大限度地减少了术前关于哪种切口能提供最佳股疝囊入路的争论,如果需要,可以改为简单的腹股沟疝修补,如果遇到需要切除的受损肠管,也可以避免进一步的皮肤切口。