Department of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, Ontario, Canada.
Cost Eff Resour Alloc. 2009 Dec 11;7:20. doi: 10.1186/1478-7547-7-20.
To evaluate cost-utility of infliximab and adalimumab for the treatment of moderate-to-severe ulcerative colitis (UC) refractory to conventional therapies in Canada.
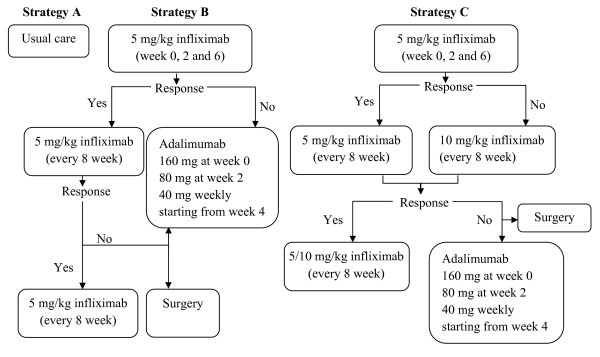
A Markov model was constructed to evaluate incremental cost-utility ratios (ICUR) of 5 mg/kg and 10 mg/kg infliximab and adalimumab therapies compared to 'usual care' in treating a hypothetical cohort of patients (aged 40 years and weighing 80 kg) over a five-year time horizon from the perspective of a publicly-funded health care system. Clinical parameters were derived from the Active Ulcerative Colitis Trials 1 and 2. Costs were obtained through provincial drug benefit plans. ICUR was the main outcome measure and both deterministic and probabilistic sensitivity analyses were conducted.
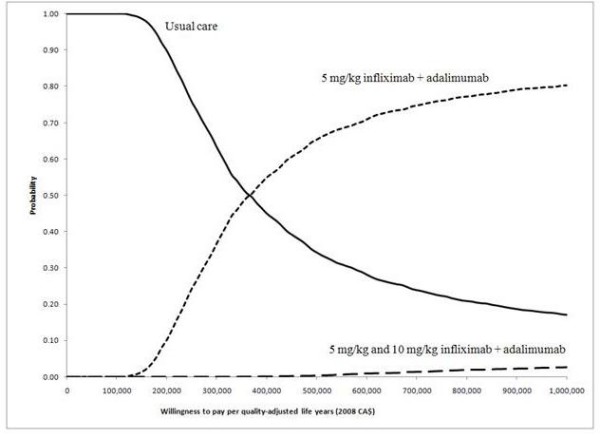
Compared to the strategy A ('usual care') in the base case analysis, the ICURs were CA$358,088/QALY for the strategy B ('5 mg/kg infliximab + adalimumab') and CA$575,540/QALY for the strategy C ('5 mg/kg and 10 mg/kg infliximab + adalimumab'). The results were sensitive to: the remission rates maintained in responders to 'usual care' and to 5 mg/kg infliximab, the rate of remission induced by adalimumab in non-responders to 5 mg/kg infliximab, early surgery rate, and utility values. When the willingness to pay (WTP) was less than CA$150,000/QALY, the probability of 'usual care' being the optimal strategy was 1.0. The probability of strategy B being optimal was 0.5 when the WTP approximated CA$400,000/QALY.
The ICURs of anti-TNF-alpha drugs were not satisfactory in treating patients with moderate-to-severe refractory UC. Future research could be aimed at the long-term clinical benefits of these drugs, especially adalimumab for patients intolerant or unresponsive to infliximab treatment.
评估英夫利昔单抗和阿达木单抗治疗对传统疗法难治的中重度溃疡性结肠炎(UC)在加拿大的成本-效用。
构建马尔可夫模型,评估在 5 年时间内,从公共资助的医疗保健系统角度来看,5mg/kg 和 10mg/kg 英夫利昔单抗和阿达木单抗治疗方案相对于“常规治疗”对假设队列中(年龄 40 岁,体重 80kg)的患者增量成本效用比(ICUR)。临床参数来自活动性溃疡性结肠炎试验 1 和 2。成本来自省级药物福利计划。ICUR 是主要的结果测量指标,并进行了确定性和概率敏感性分析。
与基础分析中的策略 A(“常规治疗”)相比,策略 B(“5mg/kg 英夫利昔单抗+阿达木单抗”)的 ICUR 为 358,088 加元/QALY,策略 C(“5mg/kg 和 10mg/kg 英夫利昔单抗+阿达木单抗”)的 ICUR 为 575,540 加元/QALY。结果对以下因素敏感:对“常规治疗”和 5mg/kg 英夫利昔单抗有反应者的缓解率、5mg/kg 英夫利昔单抗无反应者对阿达木单抗的缓解率、早期手术率和效用值。当支付意愿(WTP)低于 150,000 加元/QALY 时,“常规治疗”是最佳策略的概率为 1.0。当 WTP 接近 400,000 加元/QALY 时,策略 B 成为最佳策略的概率为 0.5。
抗 TNF-α 药物治疗中重度难治性 UC 的 ICUR 并不令人满意。未来的研究可以针对这些药物的长期临床获益,特别是对于对英夫利昔单抗治疗不耐受或无反应的患者使用阿达木单抗。