Health Policy and Management, DeGroote School of Business, McMaster University, 1280 Main Street West, Ontario, Hamilton, L8S 4M4, Canada.
BMC Health Serv Res. 2021 Nov 13;21(1):1231. doi: 10.1186/s12913-021-07260-z.
The prediction of the real-world cost of adverse drug reactions (ADRs) has historically relied on the data from randomized controlled trials (RCT). However, trial conditions do not always reflect the real-world applications of pharmaceutical products; hence, they may not accurately portray the actual risks of ADRs associated with them. The objective of this study is two-fold: (a) demonstrate whether and how post-market and RCT ADR data could lead to different conclusions for a set of drugs of interest, and (b) evaluate the potential economic impact of the post-market ADRs associated with those drugs.
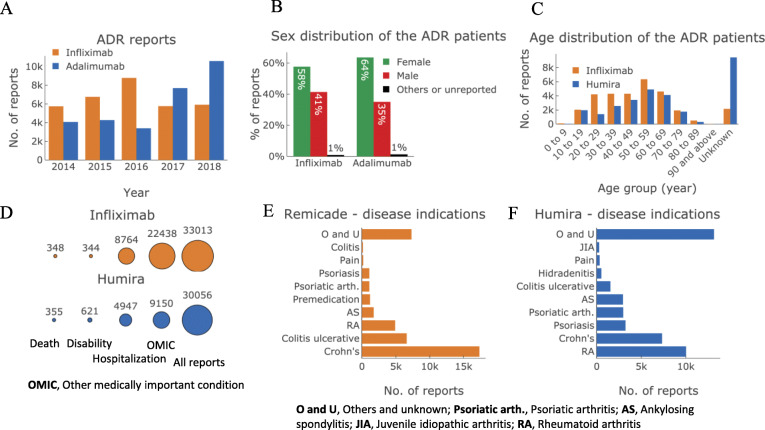
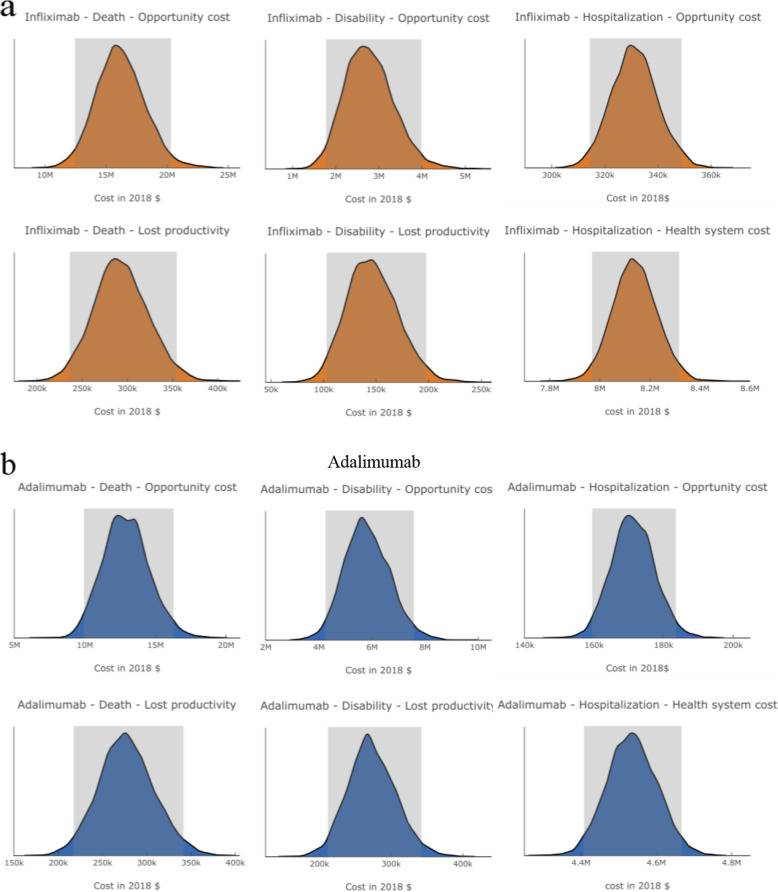
We selected two TNF-α inhibitor biologics, infliximab and adalimumab, and used the Canada Vigilance Adverse Reaction (CVAR) online database as a source of post-market ADR data. Adverse reaction data from RCTs were obtained from ClinicalTrials.gov . Direct healthcare costs associated with adverse reactions were obtained from Canadian Institute for Health Information (CIHI) or Interactive Health Data Application, Alberta. We calculated post-market ADR rates and compared them with those found in the randomized controlled trials of these two drugs. Using the post-market data, we estimated the costs associated with serious ADRs from three perspectives: patient, health system, and societal.
For both drugs, the post-market and RCT data exhibited significantly different adverse reaction rates for several different clinical outcomes. As a general trend, more serious adverse reactions, such as death, appeared to have a higher rate in post-market applications compared to the clinical trials. The estimated average annual economic burden of the severe adverse reaction outcomes ranged from $10 million to $20 million for infliximab and $6 million to $19 million for adalimumab.
The frequency and severity of post-market adverse reactions associated with pharmaceutical products may significantly differ from those detected in the clinical trials. Despite possible methodological differences, this is due to the fact that post-market data reflect the externalities of the real-world that are absent in RCTs. The economic burden of adverse reactions can be substantial, and the cost calculated using post-market data is better reflective of the cost of ADRs in the real-world.
预测药物不良反应(ADR)的实际成本在历史上一直依赖于随机对照试验(RCT)的数据。然而,试验条件并不总是反映药品的实际应用情况;因此,它们可能无法准确描述与之相关的 ADR 的实际风险。本研究的目的有两个:(a)证明在一组感兴趣的药物中,上市后和 RCT 的 ADR 数据是否以及如何得出不同的结论;(b)评估与这些药物相关的上市后 ADR 的潜在经济影响。
我们选择了两种 TNF-α 抑制剂生物制剂,英夫利昔单抗和阿达木单抗,并使用加拿大警戒不良事件在线数据库(CVAR)作为上市后 ADR 数据的来源。RCT 中的不良反应数据来自 ClinicalTrials.gov。与不良反应相关的直接医疗费用来自加拿大健康信息研究所(CIHI)或艾伯塔省互动健康数据应用程序。我们计算了上市后 ADR 率,并将其与这两种药物的随机对照试验中发现的 ADR 率进行了比较。使用上市后数据,我们从患者、医疗系统和社会三个角度估计了严重 ADR 相关的成本。
对于这两种药物,上市后和 RCT 数据在几个不同的临床结局上显示出显著不同的不良反应率。一般来说,与临床试验相比,上市后应用中似乎出现了更高比例的更严重不良反应,如死亡。英夫利昔单抗严重不良反应结局的估计平均年经济负担范围为 1000 万至 2000 万加元,阿达木单抗为 600 万至 1900 万加元。
与药品相关的上市后不良反应的频率和严重程度可能与临床试验中检测到的有显著差异。尽管可能存在方法学差异,但这是由于上市后数据反映了 RCT 中不存在的现实世界的外部性。不良反应的经济负担可能很大,并且使用上市后数据计算的成本更能反映实际世界中 ADR 的成本。