MRC Clinical Trials Unit, 222 Euston Road, London NW1 2DA, UK.
Lancet. 2010 Jan 9;375(9709):123-31. doi: 10.1016/S0140-6736(09)62067-5. Epub 2009 Dec 8.
HIV antiretroviral therapy (ART) is often managed without routine laboratory monitoring in Africa; however, the effect of this approach is unknown. This trial investigated whether routine toxicity and efficacy monitoring of HIV-infected patients receiving ART had an important long-term effect on clinical outcomes in Africa.
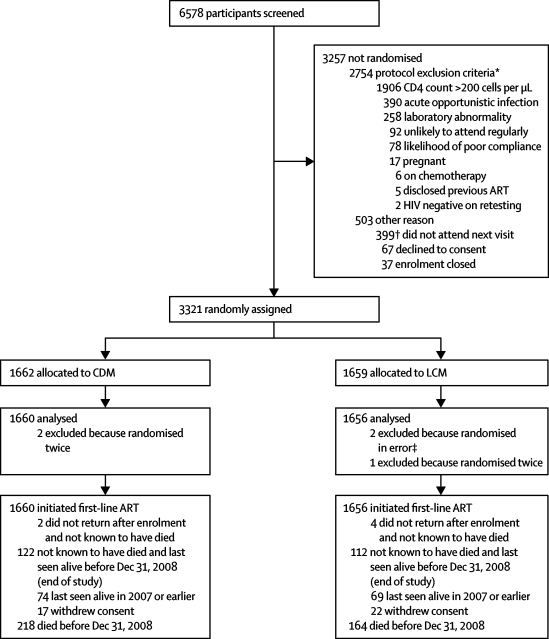
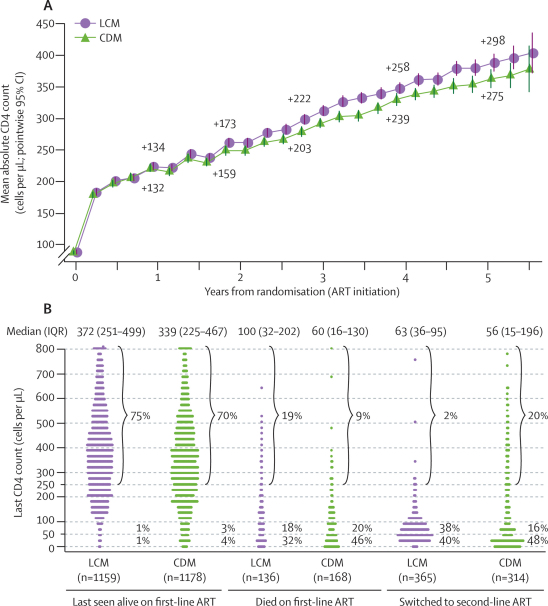
In this open, non-inferiority trial in three centres in Uganda and one in Zimbabwe, 3321 symptomatic, ART-naive, HIV-infected adults with CD4 counts less than 200 cells per microL starting ART were randomly assigned to laboratory and clinical monitoring (LCM; n=1659) or clinically driven monitoring (CDM; n=1662) by a computer-generated list. Haematology, biochemistry, and CD4-cell counts were done every 12 weeks. In the LCM group, results were available to clinicians; in the CDM group, results (apart from CD4-cell count) could be requested if clinically indicated and grade 4 toxicities were available. Participants switched to second-line ART after new or recurrent WHO stage 4 events in both groups, or CD4 count less than 100 cells per microL (LCM only). Co-primary endpoints were new WHO stage 4 HIV events or death, and serious adverse events. Non-inferiority was defined as the upper 95% confidence limit for the hazard ratio (HR) for new WHO stage 4 events or death being no greater than 1.18. Analyses were by intention to treat. This study is registered, number ISRCTN13968779.
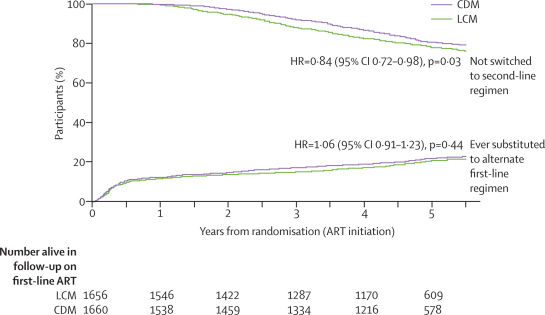
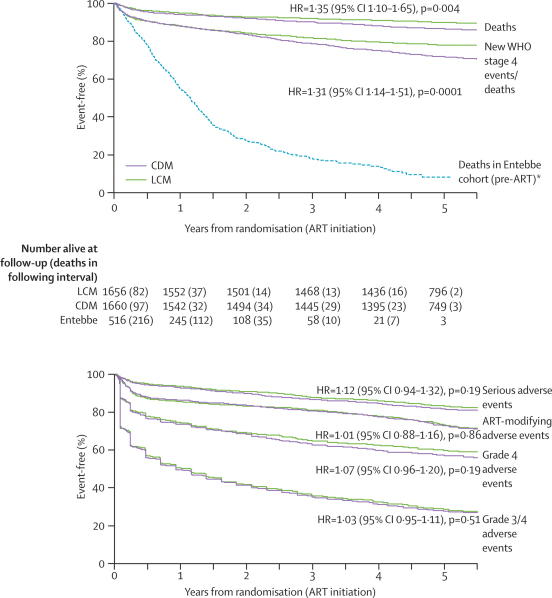
Two participants assigned to CDM and three to LCM were excluded from analyses. 5-year survival was 87% (95% CI 85-88) in the CDM group and 90% (88-91) in the LCM group, and 122 (7%) and 112 (7%) participants, respectively, were lost to follow-up over median 4.9 years' follow-up. 459 (28%) participants receiving CDM versus 356 (21%) LCM had a new WHO stage 4 event or died (6.94 [95% CI 6.33-7.60] vs 5.24 [4.72-5.81] per 100 person-years; absolute difference 1.70 per 100 person-years [0.87-2.54]; HR 1.31 [1.14-1.51]; p=0.0001). Differences in disease progression occurred from the third year on ART, whereas higher rates of switch to second-line treatment occurred in LCM from the second year. 283 (17%) participants receiving CDM versus 260 (16%) LCM had a new serious adverse event (HR 1.12 [0.94-1.32]; p=0.19), with anaemia the most common (76 vs 61 cases).
ART can be delivered safely without routine laboratory monitoring for toxic effects, but differences in disease progression suggest a role for monitoring of CD4-cell count from the second year of ART to guide the switch to second-line treatment.
UK Medical Research Council, the UK Department for International Development, the Rockefeller Foundation, GlaxoSmithKline, Gilead Sciences, Boehringer-Ingelheim, and Abbott Laboratories.
在非洲,艾滋病毒抗逆转录病毒疗法(ART)通常在没有常规实验室监测的情况下进行管理;然而,这种方法的效果尚不清楚。本试验研究了在非洲,接受 ART 的艾滋病毒感染者接受常规毒性和疗效监测是否对临床结局有重要的长期影响。
在乌干达的三个中心和津巴布韦的一个中心进行的这项开放、非劣效性试验中,3321 名有症状、初次接受 ART、CD4 计数低于 200 个细胞/微升的艾滋病毒感染成年人开始接受 ART,随机分配到实验室和临床监测(LCM;n=1659)或临床驱动监测(CDM;n=1662)组,由计算机生成的列表分配。每 12 周进行一次血液学、生物化学和 CD4 细胞计数。在 LCM 组,结果提供给临床医生;在 CDM 组,如果临床需要,可以请求结果(除 CD4 细胞计数外),并且可以获得 4 级毒性。两组参与者在新的或复发的世界卫生组织第 4 阶段事件或 CD4 计数低于 100 个细胞/微升(仅 LCM)后转换为二线 ART。主要终点是新的世界卫生组织第 4 阶段 HIV 事件或死亡和严重不良事件。非劣效性定义为新的世界卫生组织第 4 阶段事件或死亡的风险比(HR)的上限 95%置信区间不大于 1.18。分析采用意向治疗。这项研究在 ClinicalTrials.gov 注册,编号为 ISRCTN13968779。
在 CDM 组和 LCM 组中,各有两名参与者和三名参与者被排除在分析之外。CDM 组的 5 年生存率为 87%(95%CI 85-88),LCM 组为 90%(88-91),中位随访 4.9 年后,分别有 122 名(7%)和 112 名(7%)参与者失访。459 名接受 CDM 的参与者与 356 名接受 LCM 的参与者发生新的世界卫生组织第 4 阶段事件或死亡(6.94[95%CI 6.33-7.60]与 5.24[4.72-5.81]每 100 人年;绝对差值为 1.70 每 100 人年[0.87-2.54];HR 1.31[1.14-1.51];p=0.0001)。疾病进展的差异从 ART 治疗的第三年开始出现,而 LCM 组从第二年开始更频繁地转换为二线治疗。283 名接受 CDM 的参与者与 260 名接受 LCM 的参与者发生新的严重不良事件(HR 1.12[0.94-1.32];p=0.19),贫血最常见(76 例与 61 例)。
ART 可以在没有常规实验室监测毒性作用的情况下安全地提供,但疾病进展的差异表明,从 ART 的第二年开始监测 CD4 细胞计数可以指导二线治疗的转换。
英国医学研究理事会、英国国际发展部、洛克菲勒基金会、葛兰素史克、吉利德科学公司、勃林格殷格翰和雅培实验室。