Department of Medicine III, Intensive Care Unit, Medical University of Vienna, Vienna, Austria.
Diabetes Care. 2010 Mar;33(3):467-72. doi: 10.2337/dc09-1352. Epub 2009 Dec 10.
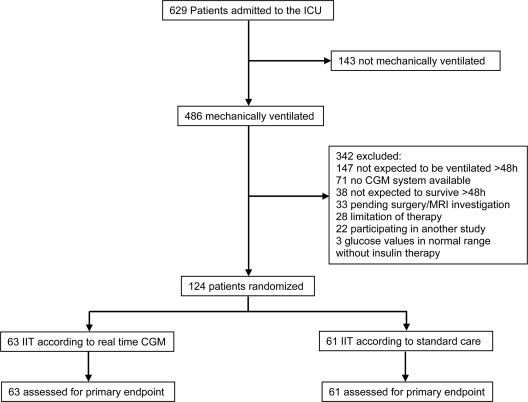
OBJECTIVE To evaluate the impact of real-time continuous glucose monitoring (CGM) on glycemic control and risk of hypoglycemia in critically ill patients. RESEARCH DESIGN AND METHODS A total 124 patients receiving mechanical ventilation were randomly assigned to the real-time CGM group (n = 63; glucose values given every 5 min) or to the control group (n = 61; selective arterial glucose measurements according to an algorithm; simultaneously blinded CGM) for 72 h. Insulin infusion rates were guided according to the same algorithm in both groups. The primary end point was percentage of time at a glucose level <110 mg/dl. Secondary end points were mean glucose levels and rate of severe hypoglycemia (<40 mg/dl). RESULTS Percentage of time at a glucose level <110 mg/dl (59.0 +/- 20 vs. 55.0 +/- 18% in the control group, P = 0.245) and the mean glucose level (106 +/- 18 vs. 111 +/- 10 mg/dl in the control group, P = 0.076) could not be improved using real-time CGM. The rate of severe hypoglycemia was lower in the real-time CGM group (1.6 vs. 11.5% in the control group, P = 0.031). CGM reduced the absolute risk of severe hypoglycemia by 9.9% (95% CI 1.2-18.6) with a number needed to treat of 10.1 (95% CI 5.4-83.3). CONCLUSIONS In critically ill patients, real-time CGM reduces hypoglycemic events but does not improve glycemic control compared with intensive insulin therapy guided by an algorithm.
评估实时连续血糖监测(CGM)对危重症患者血糖控制和低血糖风险的影响。
共纳入 124 例接受机械通气的患者,随机分为实时 CGM 组(n = 63;血糖值每 5 分钟测量一次)或对照组(n = 61;根据算法进行选择性动脉血糖测量;同时进行盲法 CGM),持续 72 小时。两组胰岛素输注率均根据相同的算法进行调整。主要终点为血糖水平<110mg/dl 的时间百分比。次要终点为平均血糖水平和严重低血糖发生率(<40mg/dl)。
血糖水平<110mg/dl 的时间百分比(实时 CGM 组为 59.0%±20%,对照组为 55.0%±18%,P=0.245)和平均血糖水平(实时 CGM 组为 106±18mg/dl,对照组为 111±10mg/dl,P=0.076)均不能通过实时 CGM 得到改善。实时 CGM 组严重低血糖发生率较低(1.6% vs. 对照组 11.5%,P=0.031)。CGM 可降低严重低血糖的绝对风险 9.9%(95%CI 1.2-18.6),需要治疗的人数为 10.1(95%CI 5.4-83.3)。
与算法指导的强化胰岛素治疗相比,实时 CGM 可降低危重症患者的低血糖事件发生率,但不能改善血糖控制。