Berger Jeffrey S, Brown David L, Burke Gregory L, Oberman Albert, Kostis John B, Langer Robert D, Wong Nathan D, Wassertheil-Smoller Sylvia
Department of Medicine, University of Pennsylvania, Philadelphia, PA 19104, USA.
Circ Cardiovasc Qual Outcomes. 2009 Mar;2(2):78-87. doi: 10.1161/CIRCOUTCOMES.108.791269. Epub 2009 Mar 5.
Despite compelling evidence that aspirin reduces fatal and nonfatal vascular events among the overall population in various settings, women have frequently been underrepresented and their data underreported. We sought to evaluate the relationship between aspirin use, dose (81 or 325 mg), and clinical outcomes among postmenopausal women with stable cardiovascular disease (CVD).
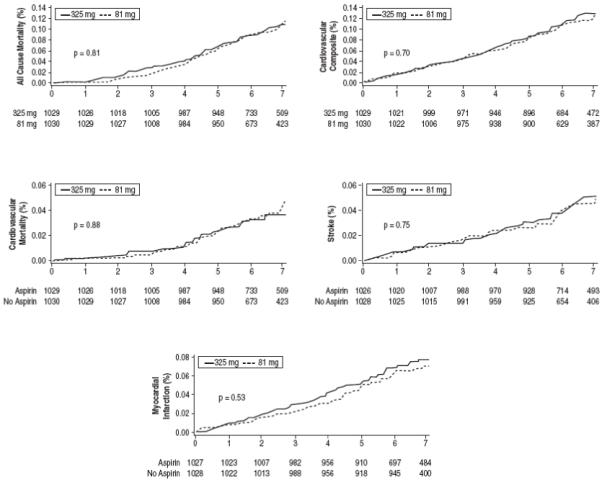
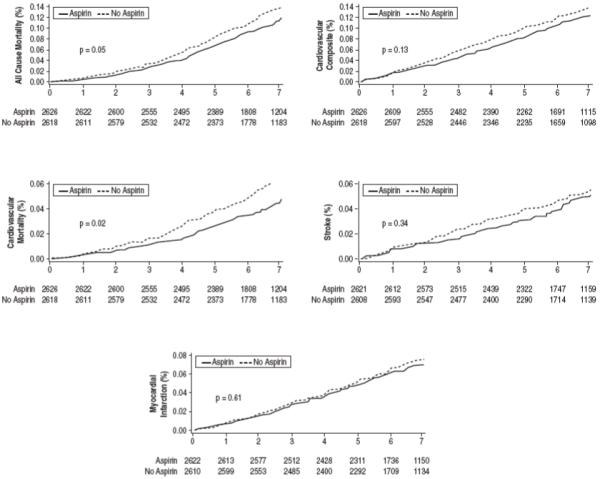
Women with CVD (n=8928) enrolled in the Women's Health Initiative Observational Study were used for this analysis. The primary outcome was the incidence of all-cause mortality and cardiovascular events (myocardial infarction, stroke, and cardiovascular death). Among 8928 women with stable CVD, 4101 (46%) reported taking aspirin, of whom 30% were on 81 mg and 70% were on 325 mg. At 6.5 years of follow-up, no significant association was noted for aspirin use and all-cause mortality or cardiovascular events. However, after multivariate adjustment, aspirin use was associated with a significantly lower all-cause (adjusted hazard ratio, 0.86 [0.75 to 0.99]; P=0.04) and cardiovascular-related mortality (adjusted hazard ratio, 0.75 [0.60 to 0.95]; P=0.01) compared with no aspirin. Aspirin use was associated with a lower risk of cardiovascular events (adjusted hazard ratio, 0.90 [0.78 to 1.04]; P=0.14), which did not meet statistical significance. Compared with 325 mg, use of 81 mg was not significantly different for all-cause mortality, cardiovascular events, or any individual end point.
After multivariate adjustment, aspirin use was associated with significantly lower risk of all-cause mortality, specifically, cardiovascular mortality, among postmenopausal women with stable CVD. No significant difference was noted between 81 mg and 325 mg of aspirin. Overall, aspirin use was low in this cohort of women with stable CVD.
尽管有确凿证据表明阿司匹林可降低不同情况下总体人群的致命和非致命血管事件风险,但女性在相关研究中的代表性常常不足,其数据报告也较少。我们旨在评估阿司匹林使用、剂量(81或325毫克)与绝经后稳定心血管疾病(CVD)女性临床结局之间的关系。
本分析使用了参与女性健康倡议观察性研究的患有CVD的女性(n = 8928)。主要结局是全因死亡率和心血管事件(心肌梗死、中风和心血管死亡)的发生率。在8928名患有稳定CVD的女性中,4101名(46%)报告服用阿司匹林,其中30%服用81毫克,70%服用325毫克。在6.5年的随访中,未发现阿司匹林使用与全因死亡率或心血管事件之间存在显著关联。然而,经过多变量调整后,与未服用阿司匹林相比,服用阿司匹林与显著降低的全因死亡率(调整后的风险比,0.86 [0.75至0.99];P = 0.04)和心血管相关死亡率(调整后的风险比,0.75 [0.60至0.95];P = 0.01)相关。阿司匹林使用与较低的心血管事件风险相关(调整后的风险比,0.90 [0.78至1.04];P = 0.14),但未达到统计学显著性。与325毫克相比,81毫克的使用在全因死亡率、心血管事件或任何单个终点方面无显著差异。
经过多变量调整后,服用阿司匹林与绝经后稳定CVD女性的全因死亡率,特别是心血管死亡率显著降低相关。81毫克和325毫克阿司匹林之间未发现显著差异。总体而言,在这组患有稳定CVD的女性中,阿司匹林的使用率较低。