Popescu Ioana, Werner Rachel M, Vaughan-Sarrazin Mary S, Cram Peter
Division of General Internal Medicine, Department of Internal Medicine, University of Iowa Carver College of Medicine, Center for Research in the Implementation of Innovative Strategies in Practice, Iowa City VA Medical Center, Iowa City, Iowa, USA.
Circ Cardiovasc Qual Outcomes. 2009 May;2(3):221-7. doi: 10.1161/CIRCOUTCOMES.108.813790. Epub 2009 May 5.
Studies suggest that most hospitals now have relatively high adherence with recommended acute myocardial infarction (AMI) process measures. Little is known about hospitals with consistently poor adherence with AMI process measures and whether these hospitals also have increased patient mortality.
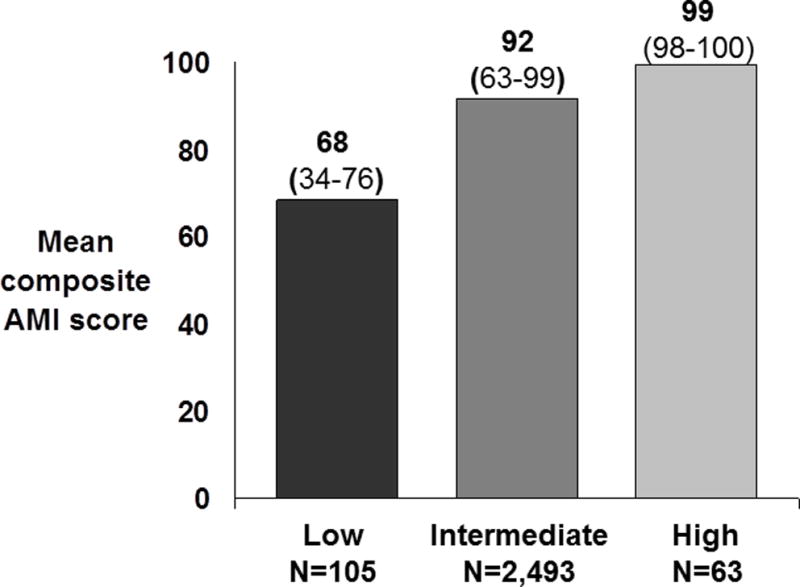
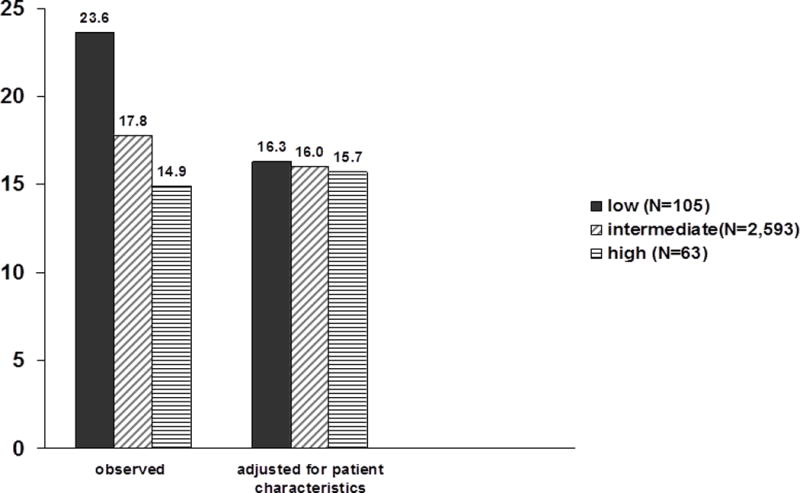
We conducted a retrospective study of 2761 US hospitals reporting AMI process measures to the Center for Medicare and Medicaid Services Hospital Compare database during 2004 to 2006 that could be linked to 2005 Medicare Part A data. The main outcome measures were hospitals' combined compliance with 5 AMI measures (aspirin and beta-blocker on admission and discharge and angiotensin-converting enzyme inhibitor/angiotensin receptor blocker use at discharge for patients with left ventricular dysfunction) and risk-adjusted 30-day mortality for 2005. We stratified hospitals into those with low AMI adherence (ranked in the lowest decile for AMI adherence for 3 consecutive years [2004-2006, n=105]), high adherence (ranked in the top decile for 3 consecutive years [n=63]), and intermediate adherence (all others [n=2593]). Mean AMI performance varied significantly across low-, intermediate-, and high-performing hospitals (mean score, 68% versus 92% versus 99%, P<0.001). Low-performing hospitals were more likely than intermediate- and high-performing hospitals to be safety-net providers (19.2% versus 11.0% versus 6.4%; P=0.005). Low-performing hospitals had higher unadjusted 30-day mortality rates (23.6% versus 17.8% versus 14.9%; P<0.001). These differences persisted after adjustment for patient characteristics (16.3% versus 16.0% versus 15.7%; P=0.02).
Consistently low-performing hospitals differ substantially from other US hospitals. Targeting quality improvement efforts toward these hospitals may offer an attractive opportunity for improving AMI outcomes.
研究表明,如今大多数医院对推荐的急性心肌梗死(AMI)诊疗流程措施的依从性相对较高。对于那些对AMI诊疗流程措施的依从性一直较差的医院,以及这些医院的患者死亡率是否也有所增加,我们了解得很少。
我们对2004年至2006年期间向医疗保险和医疗补助服务中心医院比较数据库报告AMI诊疗流程措施且可与2005年医疗保险A部分数据相链接的2761家美国医院进行了一项回顾性研究。主要结局指标为医院对5项AMI措施的综合依从性(入院和出院时使用阿司匹林和β受体阻滞剂,以及左心室功能不全患者出院时使用血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂)和2005年经风险调整的30天死亡率。我们将医院分为AMI依从性低的医院(2004 - 2006年连续3年在AMI依从性排名中处于最低十分位[n = 105])、依从性高的医院(连续3年在排名中处于最高十分位[n = 63])和依从性中等医院(其他所有医院[n = 2593])。低、中、高绩效医院的平均AMI表现差异显著(平均得分分别为68%、92%和99%,P < 0.001)。与中、高绩效医院相比,低绩效医院更有可能是安全网提供者(19.2%对11.0%对6.4%;P = 0.005)。低绩效医院未经调整的30天死亡率更高(23.6%对17.8%对14.9%;P < 0.001)。在对患者特征进行调整后这些差异仍然存在(16.3%对16.0%对15.7%;P = 0.02)。
绩效一直较低的医院与美国其他医院有很大不同。针对这些医院开展质量改进工作可能为改善AMI治疗结果提供一个有吸引力的机会。