Department of Medicine, Universidade da Região de Joinville (Univille) - Joinville/SC, Brazil.
Clinics (Sao Paulo). 2010 Feb;65(2):189-94. doi: 10.1590/S1807-59322010000200011.
To test the hypothesis that pulse pressure respiratory variation (PPV) amplification, observed in hypovolemia, can also be observed during sodium nitroprusside (SNP)-induced vasodilation.
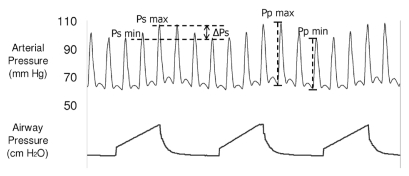
PPV is largely used for early identification of cardiac responsiveness, especially when hypovolemia is suspected. PPV results from respiratory variation in transpulmonary blood flow and reflects the left ventricular preload variations during respiratory cycles. Any factor that decreases left ventricular preload can be associated with PPV amplification, as seen in hypovolemia.
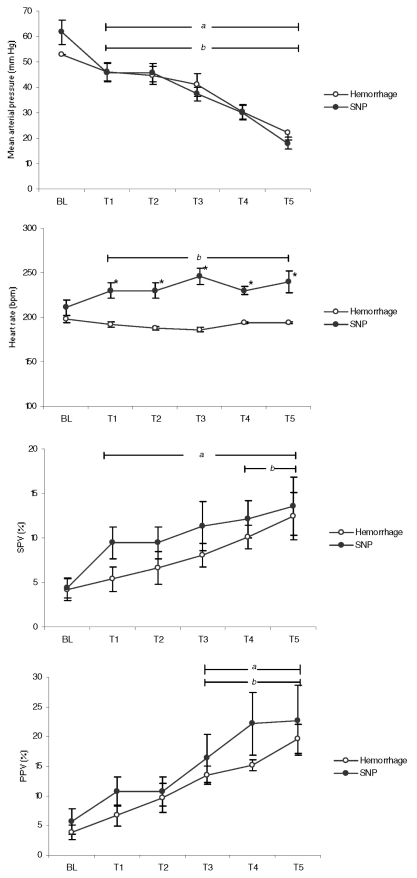
Ten anesthetized and mechanically ventilated rabbits underwent progressive hypotension by either controlled hemorrhage (Group 1) or intravenous SNP infusion (Group 2). Animals in Group 1 (n = 5) had graded hemorrhage induced at 10% steps until 50% of the total volume was bled. Mean arterial pressure (MAP) steps were registered and assumed as pressure targets to be reached in Group 2. Group 2 (n = 5) was subjected to a progressive SNP infusion to reach similar pressure targets as those defined in Group 1. Heart rate (HR), systolic pressure variation (SPV) and PPV were measured at each MAP step, and the values were compared between the groups.
SPV and PPV were similar between the experimental models in all steps (p > 0.16). SPV increased earlier in Group 2.
Both pharmacologic vasodilation and graded hemorrhage induced PPV amplification similar to that observed in hypovolemia, reinforcing the idea that amplified arterial pressure variation does not necessarily represent hypovolemic status but rather potential cardiovascular responsiveness to fluid infusion.
验证假设,即在低血容量时观察到的脉压呼吸变化(PPV)放大,也可在硝普钠(SNP)诱导的血管扩张期间观察到。
PPV 主要用于早期识别心脏反应性,尤其是在怀疑低血容量时。PPV 源自跨肺血流的呼吸变化,反映左心室前负荷在呼吸周期中的变化。任何降低左心室前负荷的因素都可能与 PPV 放大相关,如在低血容量时所见。
十只麻醉和机械通气的兔子通过控制性出血(第 1 组)或静脉注射 SNP 输注(第 2 组)进行逐渐低血压。第 1 组(n = 5)中的动物以 10%的步骤进行分级出血,直到出血总量的 50%。记录平均动脉压(MAP)步骤,并将其作为第 2 组要达到的压力目标。第 2 组(n = 5)接受逐渐 SNP 输注以达到与第 1 组定义的类似的压力目标。在每个 MAP 步骤测量心率(HR)、收缩压变化(SPV)和 PPV,并比较两组之间的值。
在所有步骤中,SPV 和 PPV 在实验模型之间相似(p > 0.16)。第 2 组中的 SPV 更早增加。
药物性血管扩张和分级出血均诱导与低血容量时观察到的类似的 PPV 放大,这强化了动脉压变化放大不一定代表低血容量状态,而是对液体输注潜在的心血管反应性的观点。