Department of Orthopaedic Surgery, Dongsan Medical Center, Keimyung University College of Medicine, Daegu, Korea.
Clin Orthop Surg. 2010 Mar;2(1):55-8. doi: 10.4055/cios.2010.2.1.55. Epub 2010 Feb 4.
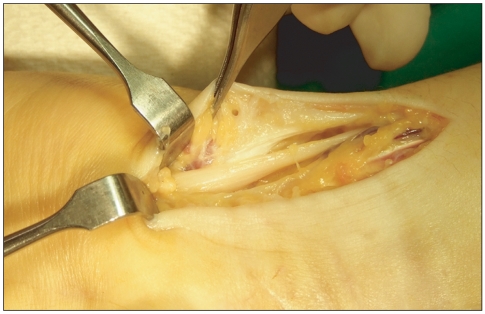
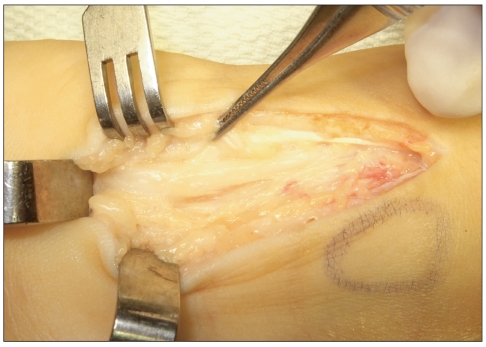
Ulnar nerve palsy subsequent to a fracture of the distal radius is extremely rare compared to a median nerve injury. The lesion tends to occur in younger patents with a high-energy mechanism of injury and a severe injury pattern consisting of wide displacement, comminution, combined distal ulnar fracture and open fracture. The mechanism of injury can contribute to a direct contusion and traction, compression secondary to prolonged edema and tissue fibrosis, intraneural fibrosis and laceration. We report 2 cases of progressive ulnar nerve palsy subsequent to closed fractures of the distal radius. The neurological symptoms recovered in all cases who underwent nerve decompression and neurolysis at 2 or 3 months after the trauma. It is recommended that cases with high-energy, widely displaced or comminuted fractures of the distal radius be evaluated carefully for ulnar nerve as well as median nerve injury.
与正中神经损伤相比,尺神经麻痹继发于桡骨远端骨折的情况极其少见。这种损伤往往发生在年轻、高能量损伤机制和严重损伤模式的患者中,包括广泛移位、粉碎、合并尺骨远端骨折和开放性骨折。损伤机制可导致直接挫伤和牵引、长时间水肿和组织纤维化、神经内纤维化和裂伤导致的压迫。我们报告了 2 例闭合性桡骨远端骨折后进行性尺神经麻痹的病例。所有病例在创伤后 2 或 3 个月行神经减压和神经松解术,神经症状均恢复。建议对高能量、广泛移位或粉碎性桡骨远端骨折的病例仔细评估尺神经和正中神经损伤。