Princess Margaret Hospital Phase II Consortium, University of Toronto, Ontario, Canada.
Mol Cancer Ther. 2010 Mar;9(3):751-60. doi: 10.1158/1535-7163.MCT-09-0868. Epub 2010 Mar 2.
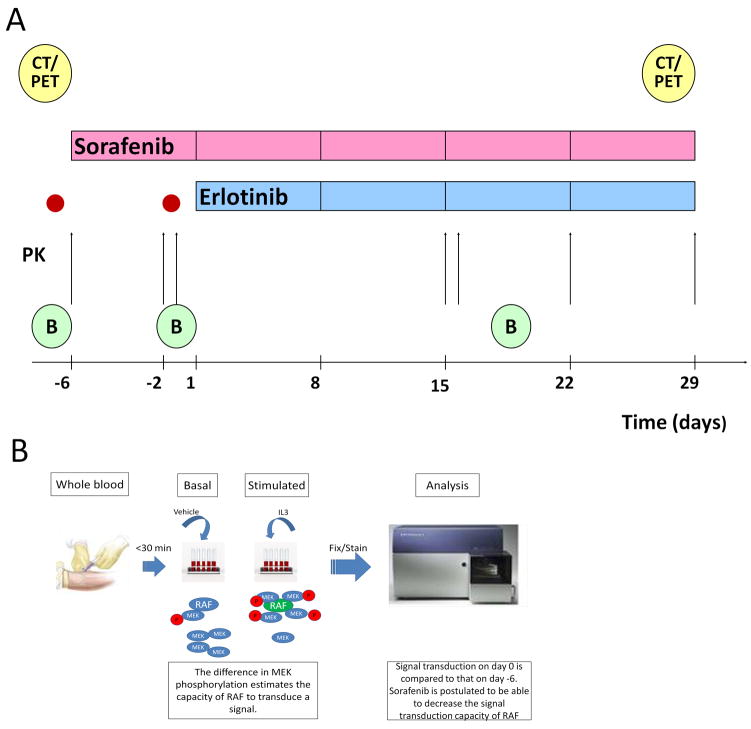
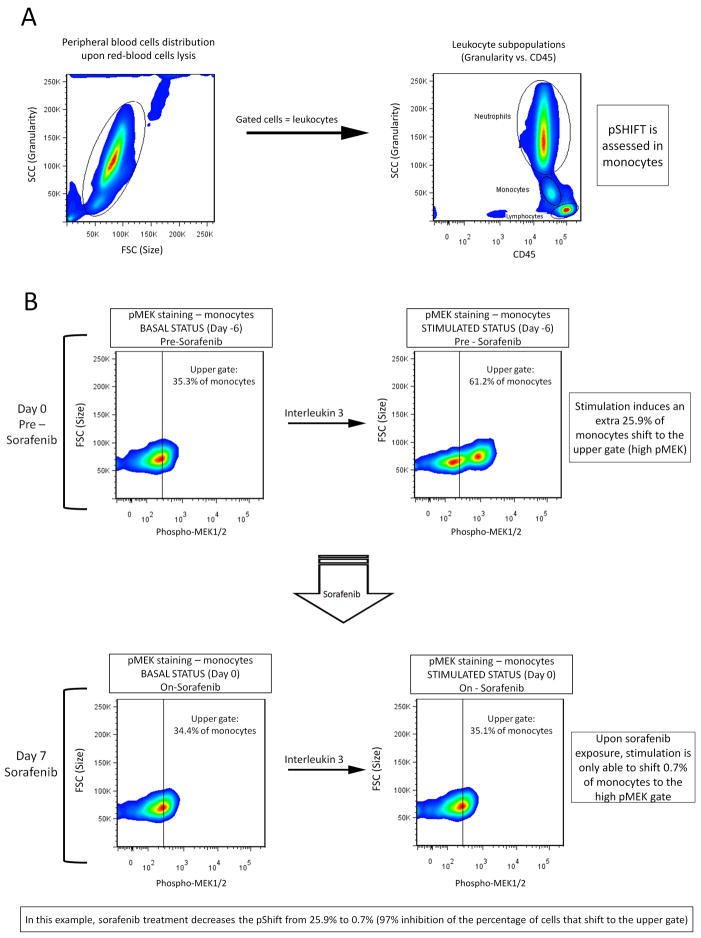
The aims of this study were to further define the safety of sorafenib and erlotinib, given at their full approved monotherapy doses, and to correlate pharmacokinetic and pharmacodynamic markers with clinical outcome. In addition, a novel pharmacodynamic marker based on the real-time measurement of RAF signal transduction capacity (STC) is described. Sorafenib was administered alone for a 1-week run-in period, and then both drugs were given together continuously. RAF STC was assessed in peripheral blood monocytes prior to erlotinib initiation. Epidermal growth factor receptor (EGFR) expression and K-RAS mutations were measured in archival tumor samples. Changes in pERK and CD31 were determined in fresh tumor biopsies obtained pretreatment, prior to erlotinib dosing, and during the administration of both drugs. In addition, positron emission tomography-computed tomography scans and pharmacokinetic assessments were done. Eleven patients received a total of 57 cycles (median, 5; range, 1-10). Only four patients received full doses of both drugs for the entire study course, with elevation of liver enzymes being the main reason for dose reductions and delays. Among 10 patients evaluable for response, 8 experienced tumor stabilization of >or=4 cycles. Pharmacokinetic analysis revealed no significant interaction of erlotinib with sorafenib. Sorafenib-induced decrease in RAF-STC showed statistically significant correlation with time-to-progression in seven patients. Other pharmacodynamic markers did not correlate with clinical outcome. This drug combination resulted in promising clinical activity in solid tumor patients although significant toxicity warrants close monitoring. RAF-STC deserves further study as a predictive marker for sorafenib.
本研究旨在进一步明确索拉非尼和厄洛替尼在全剂量单药治疗时的安全性,并将药代动力学和药效学标志物与临床结果相关联。此外,还描述了一种基于 RAF 信号转导能力(STC)实时测量的新型药效学标志物。索拉非尼先单独给药 1 周作为导入期,然后两种药物连续同时给药。在厄洛替尼开始前,检测外周血单核细胞中的 RAF STC。检测存档肿瘤样本中的表皮生长因子受体(EGFR)表达和 K-RAS 突变。在获得预处理、厄洛替尼给药前和两种药物给药期间的新鲜肿瘤活检中,测定 pERK 和 CD31 的变化。此外,还进行了正电子发射断层扫描-计算机断层扫描扫描和药代动力学评估。11 名患者共接受了 57 个周期的治疗(中位数为 5;范围,1-10)。只有 4 名患者在整个研究过程中接受了两种药物的全剂量治疗,主要因肝酶升高而减少和延迟剂量。在 10 名可评估反应的患者中,有 8 名患者的肿瘤稳定期>或=4 个周期。药代动力学分析显示,厄洛替尼与索拉非尼之间无显著相互作用。在 7 名患者中,索拉非尼诱导的 RAF-STC 降低与无进展时间具有统计学显著相关性。其他药效学标志物与临床结果无相关性。尽管毒性显著需要密切监测,但这种药物联合治疗在实体瘤患者中显示出有前景的临床活性。RAF-STC 作为索拉非尼的预测标志物值得进一步研究。