Public Health and HIV Section, United Nations High Commissioner for Refugees, Geneva, Switzerland.
Confl Health. 2010 Jan 29;4:2. doi: 10.1186/1752-1505-4-2.
Access to HIV and malaria control programmes for refugees and internally displaced persons (IDPs) is not only a human rights issue but a public health priority for affected populations and host populations. The primary source of funding for malaria and HIV programmes for many countries is the Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund). This article analyses the current HIV and malaria National Strategic Plans (NSPs) and Global Fund approved proposals from rounds 1-8 for countries in Africa hosting populations with refugees and/or IDPs to document their inclusion.
The review was limited to countries in Africa as they constitute the highest caseload of refugees and IDPs affected by HIV and malaria. Only countries with a refugee and/or IDP population of > or = 10,000 persons were included. NSPs were retrieved from primary and secondary sources while approved Global Fund proposals were obtained from the organisation's website. Refugee figures were obtained from the United Nations High Commissioner for Refugees' database and IDP figures from the Internal Displacement Monitoring Centre. The inclusion of refugees and IDPs was classified into three categories: 1) no reference; 2) referenced; and 3) referenced with specific activities.
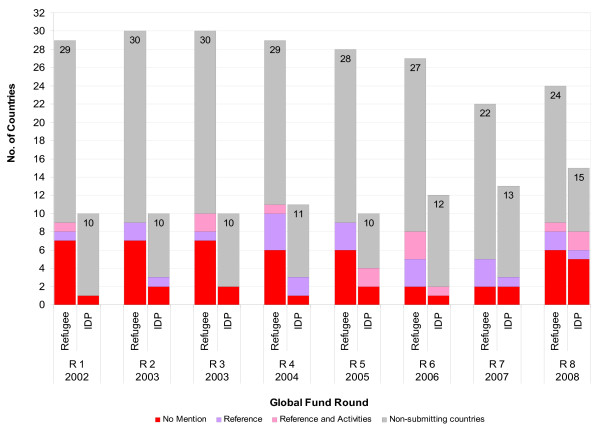
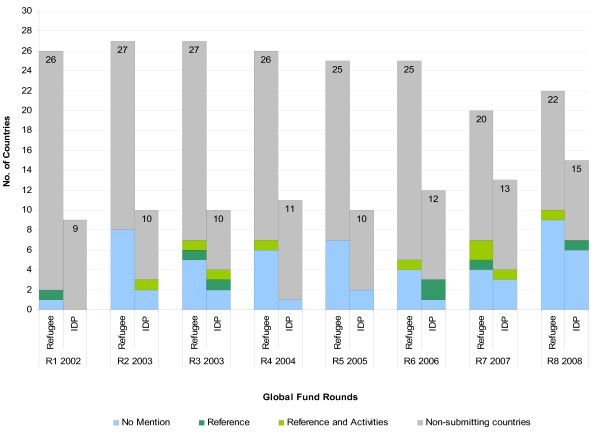
A majority of countries did not mention IDPs (57%) compared with 48% for refugees in their HIV NSPs. For malaria, refugees were not included in 47% of NSPs compared with 44% for IDPs. A minority (21-29%) of HIV and malaria NSPs referenced and included activities for refugees and IDPs. There were more approved Global Fund proposals for HIV than malaria for countries with both refugees and IDPs, respectively. The majority of countries with > or =10,000 refugees and IDPs did not include these groups in their approved proposals (61%-83%) with malaria having a higher rate of exclusion than HIV.
Countries that have signed the 1951 refugee convention have an obligation to care for refugees and this includes provision of health care. IDPs are citizens of their own country but like refugees may also not be a priority for Governments' NSPs and funding proposals. Besides legal obligations, Governments have a public health imperative to include these groups in NSPs and funding proposals. Governments may wish to add a component for refugees that is additional to the needs for their own citizens. The inclusion of forcibly displaced persons in funding proposals may have positive direct effects for host populations as international and United Nations agencies often have strong logistical capabilities that could benefit both populations. For NSPs, strong and concerted advocacy at global, regional and country levels needs to occur to successfully ensure that affected populations are included in their plans. It is essential for their inclusion to occur if we are to reach the stated goal of universal access and the Millennium Development Goals.
为难民和国内流离失所者(IDP)提供艾滋病毒和疟疾控制方案不仅是一项人权问题,也是受影响人群和收容人群的公共卫生重点。许多国家疟疾和艾滋病毒方案的主要资金来源是全球抗击艾滋病、结核病和疟疾基金(全球基金)。本文分析了非洲收容难民和/或 IDP 人口的国家在第 1-8 轮中当前的艾滋病毒和疟疾国家战略计划(NSP)和全球基金批准的提案,以记录其纳入情况。
审查仅限于非洲国家,因为它们是受艾滋病毒和疟疾影响的难民和 IDP 人数最多的国家。只包括难民和/或 IDP 人数超过或等于 10,000 人的国家。NSP 可从主要和次要来源中检索,而批准的全球基金提案可从该组织的网站上获得。难民人数来自联合国难民事务高级专员数据库,国内流离失所者人数来自国内流离失所监测中心。难民和 IDP 的纳入情况分为三类:1)无提及;2)提及;3)提及并开展具体活动。
在艾滋病毒 NSP 中,与 IDP 相比,大多数国家未提及 IDP(57%),而提及难民的比例为 48%。在疟疾方面,47%的 NSP 未提及难民,而 IDP 的比例为 44%。只有少数(21-29%)的艾滋病毒和疟疾 NSP 提及并开展了针对难民和 IDP 的活动。在有难民和 IDP 的国家中,获得全球基金批准的艾滋病毒提案多于疟疾,分别为。在有超过或等于 10,000 名难民和 IDP 的国家中,大多数国家没有将这些群体纳入其批准的提案中(61%-83%),其中疟疾的排除率高于艾滋病毒。
签署 1951 年《难民公约》的国家有照顾难民的义务,包括提供医疗保健。国内流离失所者是本国公民,但与难民一样,他们也可能不是政府 NSP 和供资提案的优先事项。除法律义务外,政府还有一项公共卫生要务,即将这些群体纳入 NSP 和供资提案中。政府可能希望为难民增加一个除本国公民需求以外的组成部分。在供资提案中纳入被迫流离失所者可能会对收容国人口产生积极的直接影响,因为国际和联合国机构通常具有强大的后勤能力,这可能使两国人口都受益。为了成功确保受影响人群被纳入其计划,需要在全球、区域和国家各级进行强有力和协调一致的宣传。如果我们要实现普及获取和千年发展目标,那么必须将他们纳入其中。