Klinik für Radiologie und Nuklearmedizin, Universitätsklinikum Magdeburg, Otto-von-Guericke-Universität Magdeburg, Germany.
Radiat Oncol. 2010 Mar 24;5:24. doi: 10.1186/1748-717X-5-24.
Micrometastases of colorectal liver metastases are present in up to 50% of lesions. In this study we sought to determine the threshold dose for local control of occult micrometastases in patients undergoing CT (computed tomography)-guided brachytherapy of colorectal liver metastases.
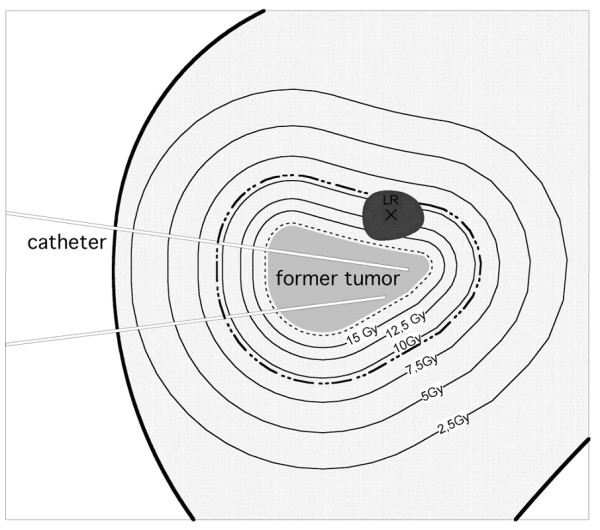
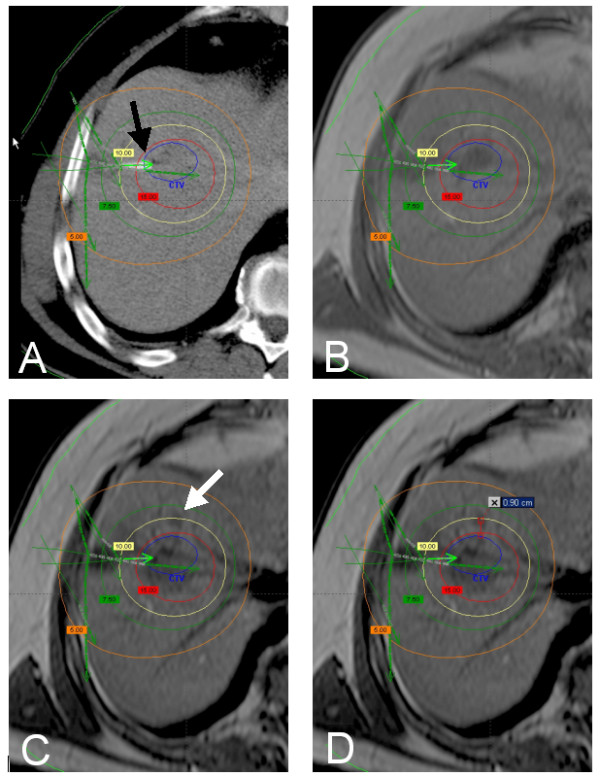
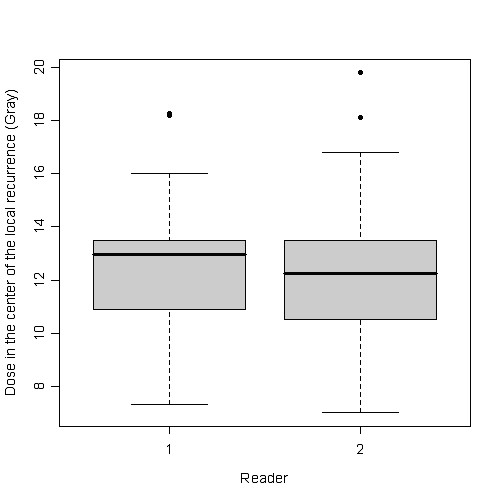
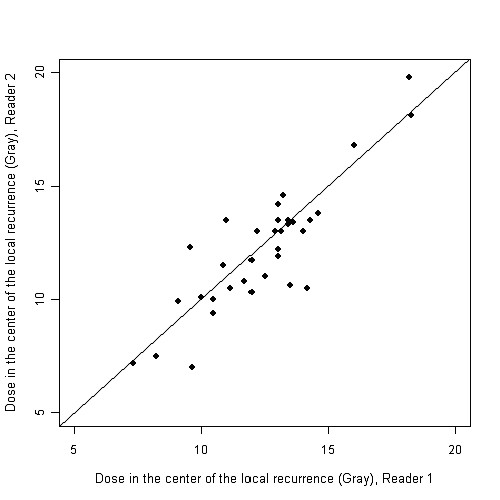
Nineteen patients demonstrated 34 local tumor recurrences originating from micrometastases after CT-guided brachytherapy of 27 colorectal liver metastases. We considered a local tumor recurrence as originating from a micrometastasis if tumor regrowth occurred adjacent to a formerly irradiated lesion and the distance of the 3D isocenter of the new lesion was <or= 23.5 mm from the previous tumor margin. Follow-up MRI was fused with the planning-CT and dosimetry data. Two reviewers independently indicated the dose exposure at the isocenter of the micrometastases. Statistical analysis included an analysis of variance (ANOVA) using backward selection. 95% tolerance intervals with coverage of 87.5 and 75% of the data of the normal distribution were calculated.
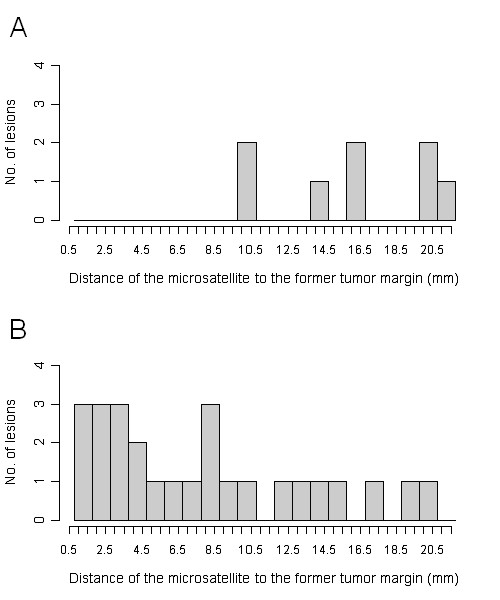
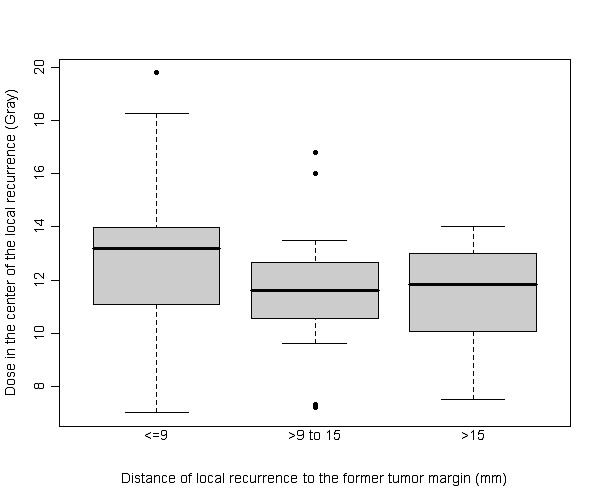
The median distance of the micrometastases to the margin of the originating colorectal metastases was 8.75 mm (1-21 mm). Dose exposure at the isocenter was 12.25 Gy (7-19.8) in median. We stratified according to the distance from the isocenter to the initial tumor margin: <or= 9 mm, > 9-15 mm and > 15 mm. The median dose in the according isocenters was 13.18, 11.6 and 11.85 Gy. The threshold dose failing to prevent micrometastasis growth was sigificantly higher in a subgroup of lesions with <or= 9 mm distance as compared to > 15 mm (13.18 vs 11.85 Gy). Adjuvant chemotherapy correlated with greater distance of micrometastasis growth to the tumor but not with the threshold dose.
To prevent loss of local tumor control by continuous growth of micrometastases a threshold dose of 15,4 Gy (single fraction) should be delivered at a distance of 21 mm to the gross tumor margin.
结直肠癌肝转移的微转移灶的存在率高达 50%。本研究旨在确定 CT 引导下结直肠癌肝转移瘤近距离放疗中隐匿性微转移灶局部控制的阈值剂量。
19 例患者在 27 例结直肠癌肝转移 CT 引导下近距离放疗后出现 34 处源于微转移灶的局部肿瘤复发。如果肿瘤复发发生在以前照射过的病变旁,且新病变的三维等中心与前肿瘤边界的距离≤23.5mm,我们认为局部肿瘤复发源于微转移灶。将 MRI 随访与计划 CT 和剂量学数据融合。两名审查员独立标记微转移灶等中心的剂量暴露。统计分析包括使用向后选择的方差分析(ANOVA)。计算了正态分布数据的 95%容忍区间,其覆盖范围为 87.5%和 75%。
微转移灶与起源于结直肠癌转移灶边缘的中位数距离为 8.75mm(1-21mm)。等中心剂量中位数为 12.25Gy(7-19.8Gy)。我们根据等中心到初始肿瘤边界的距离进行分层:≤9mm、>9-15mm 和>15mm。相应等中心的中位剂量分别为 13.18Gy、11.6Gy 和 11.85Gy。距离≤9mm的亚组中,阻止微转移灶生长的阈值剂量明显高于距离>15mm的亚组(13.18Gy 与 11.85Gy)。辅助化疗与微转移灶生长距离肿瘤较远相关,但与阈值剂量无关。
为了防止微转移灶连续生长导致局部肿瘤控制失败,应在肿瘤外 21mm 处给予 15.4Gy(单次剂量)的阈值剂量。