INSERM U897, France.
AIDS. 2010 Apr 24;24(7):1043-50. doi: 10.1097/qad.0b013e3283377a06.
To compare the lymphocyte T CD4+ (CD4) response to combinations of antiretroviral therapy (ART) in HIV-1, HIV-2 and dually positive patients in West Africa.
Collaboration of 12 prospective cohorts of HIV-infected adults followed in Senegal (2), Gambia (1), Mali (2), Benin (1) and Côte d'Ivoire (6).
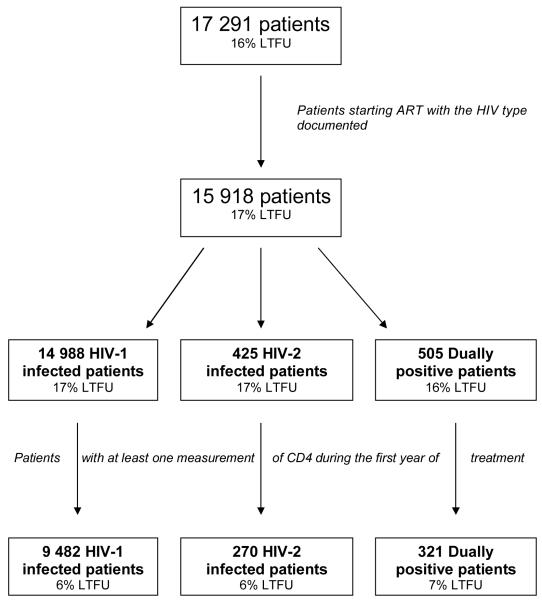
Nine thousand, four hundred and eighty-two patients infected by HIV-1 only, 270 by HIV-2 only and 321 dually positive, who initiated an ART.
CD4 change over a 12-month period.
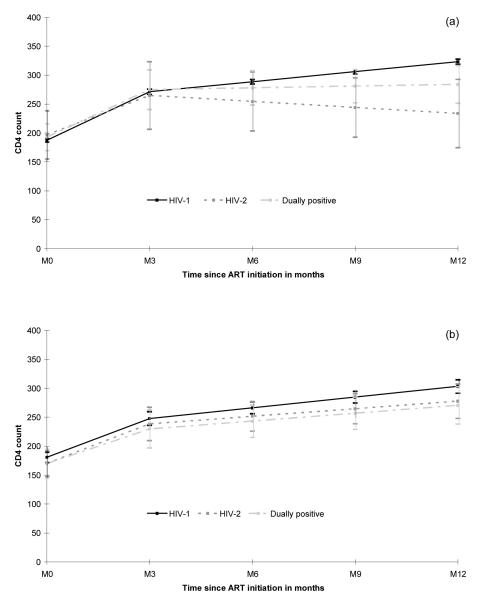
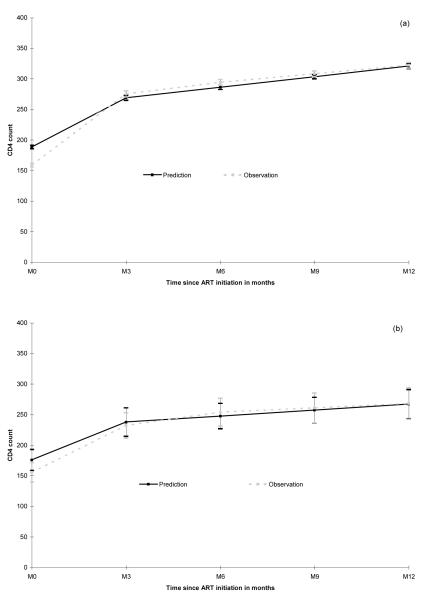
Observed CD4 cell counts at treatment initiation were similar in the three groups [overall median 155, interquartile range (IQR) 68; 249 cells/microl). In HIV-1 patients, the most common ART regimen was two nucleoside reverse transcriptase inhibitors (NRTIs) and one non-nucleoside reverse transcriptase inhibitor (NNRTI; N = 7714) as well as for dually positive patients (N = 135). HIV-2 patients were most often treated with a protease inhibitor-based regimen (N = 193) but 45 of them were treated with an NNRTI-containing ART. In those treated with a NNRTI-containing regimen, the estimated mean CD4 change between 3 and 12 months was significantly lower in HIV-2 (-41 cells/microl per year) and dually positive patients (+12 cells/microl per year) compared to HIV-1 patients (+69 cells/microl per year, overall P value 0.01). The response in HIV-2 and dually positive patients treated by another regimen (triple NRTIs or protease inhibitor-containing ART) was not significantly different than the response obtained in HIV-1-only patients (all P values >0.30).
An optimal CD4 response to ART in West Africa requires determining HIV type prior to initiation of antiretroviral drugs. NNRTIs are the mainstay of first-line ART in West Africa but are not adapted to the treatment of HIV-2 and dually positive patients.
比较在西非感染 HIV-1、HIV-2 及混合感染患者中,不同抗逆转录病毒治疗(ART)方案对淋巴细胞 T 细胞 CD4+(CD4)的影响。
协作的 12 个前瞻性队列研究包括在塞内加尔(2)、冈比亚(1)、马里(2)、贝宁(1)和科特迪瓦(6)随访的感染 HIV-1 的成年患者。
9482 例仅感染 HIV-1、270 例仅感染 HIV-2 和 321 例混合感染患者,他们均开始了 ART 治疗。
12 个月期间 CD4 变化。
治疗开始时观察到的 CD4 细胞计数在三组间相似[总体中位数 155,四分位间距(IQR)68;249 个/微升]。在 HIV-1 患者中,最常见的 ART 方案是两种核苷逆转录酶抑制剂(NRTIs)加一种非核苷逆转录酶抑制剂(NNRTI;N=7714),双重感染患者也是如此(N=135)。HIV-2 患者最常接受基于蛋白酶抑制剂的方案治疗(N=193),但其中 45 例接受含 NNRTI 的 ART 治疗。在接受含 NNRTI 的方案治疗的患者中,与 HIV-1 患者相比(总体 P 值<0.01),HIV-2(-41 个/微升/年)和双重感染患者(+12 个/微升/年)的 CD4 估计平均变化在 3 至 12 个月期间明显更低。接受另一种方案(三 NRTIs 或含蛋白酶抑制剂的 ART)治疗的 HIV-2 和双重感染患者的反应与仅 HIV-1 患者的反应无显著差异(所有 P 值均>0.30)。
在西非,为实现 ART 的最佳 CD4 反应,需要在开始抗逆转录病毒药物之前确定 HIV 类型。NNRTI 是西非一线 ART 的主要药物,但不适合治疗 HIV-2 和双重感染患者。