Department of Neurology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA 02215, USA.
Ann Neurol. 2010 Apr;67(4):534-41. doi: 10.1002/ana.21952.
To describe the natural history, clinical, neurophysiological, and histological features, and outcomes of diabetic patients presenting with acute painful neuropathy associated with glycemic control, also referred to as insulin neuritis.
Sixteen subjects presenting with acute painful neuropathy had neurological and retinal examinations, laboratory studies, autonomic testing, and pain assessments over 18 months. Eight subjects had skin biopsies for evaluation of intraepidermal nerve fiber density.
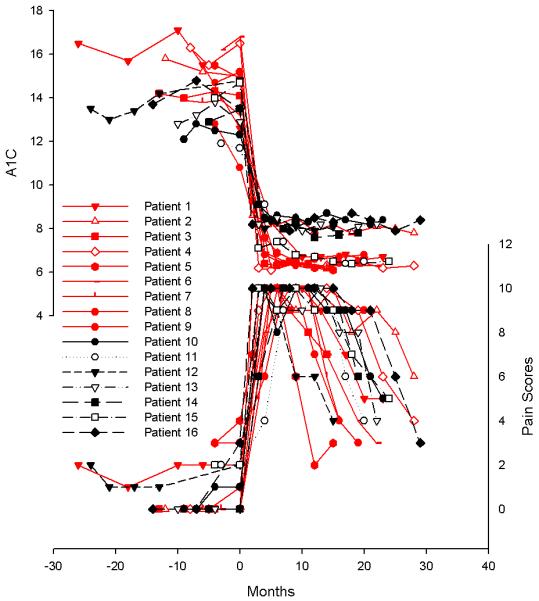
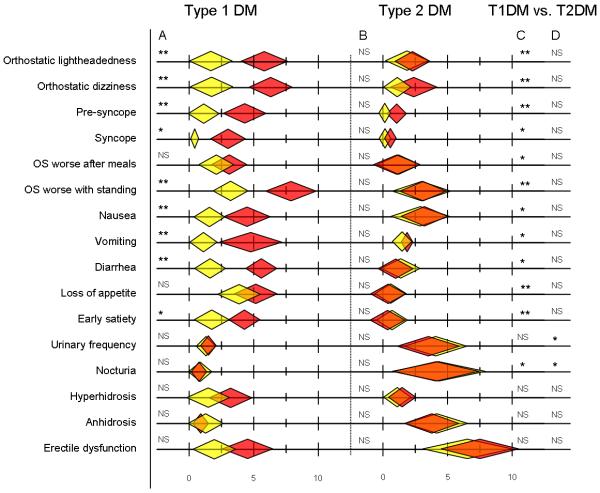
All subjects developed severe pain within 8 weeks of intensive glucose control. There was a high prevalence of autonomic cardiovascular, gastrointestinal, genitourinary, and sudomotor symptoms in all subjects. Orthostatic hypotension and parasympathetic dysfunction were seen in 69% of subjects. Retinopathy worsened in all subjects. Reduced intraepidermal nerve fiber density (IENFD) was seen in all tested subjects. After 18 months of glycemic control, there were substantial improvements in pain, autonomic symptoms, autonomic test results, and IENFD. Greater improvements were seen after 18 months in type 1 versus type 2 diabetic subjects in autonomic symptoms (cardiovascular p < 0.01; gastrointestinal p < 0.01; genitourinary p < 0.01) and autonomic function tests (p < 0.01, sympathetic and parasympathetic function tests).
Treatment-induced neuropathy is characterized by acute, severe pain, peripheral nerve degeneration, and autonomic dysfunction after intensive glycemic control. The neuropathy occurred in parallel with worsening diabetic retinopathy, suggesting a common underlying pathophysiological mechanism. Clinical features and objective measures of small myelinated and unmyelinated nerve fibers can improve in these diabetic patients despite a prolonged history of poor glucose control, with greater improvement seen in patients with type 1 diabetes.
描述与血糖控制相关的急性痛性多发性神经病(也称胰岛素神经炎)患者的自然病史、临床、神经生理学和组织学特征及结局。
16 例新发急性痛性多发性神经病患者接受了 18 个月的神经学和视网膜检查、实验室研究、自主神经测试和疼痛评估。8 例患者接受了皮肤活检,以评估表皮内神经纤维密度。
所有患者在强化血糖控制后 8 周内均出现严重疼痛。所有患者均存在自主心血管、胃肠道、泌尿生殖和汗腺症状的高患病率。69%的患者存在体位性低血压和副交感神经功能障碍。所有患者的视网膜病变均加重。所有测试患者的表皮内神经纤维密度(IENFD)均降低。在血糖控制 18 个月后,疼痛、自主症状、自主测试结果和 IENFD 均有显著改善。与 2 型糖尿病患者相比,1 型糖尿病患者在自主症状(心血管,p<0.01;胃肠道,p<0.01;泌尿生殖,p<0.01)和自主功能测试(交感和副交感功能测试,p<0.01)方面的改善更为显著。
治疗诱导的多发性神经病的特征为强化血糖控制后出现急性、严重疼痛、周围神经退行性变和自主神经功能障碍。该神经病与糖尿病视网膜病变恶化同时发生,提示存在共同的潜在病理生理机制。尽管存在长期血糖控制不佳的病史,但这些糖尿病患者的小髓鞘和无髓鞘神经纤维的临床特征和客观测量仍可改善,其中 1 型糖尿病患者的改善更为显著。