Neuroendocrine Clinical Center, Massachusetts General Hospital, Boston, USA.
BMC Endocr Disord. 2010 May 17;10:10. doi: 10.1186/1472-6823-10-10.
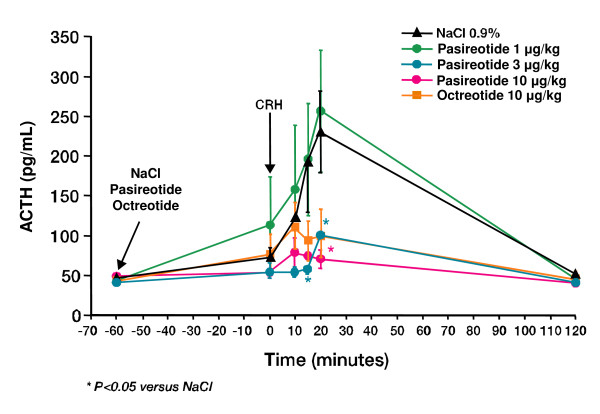
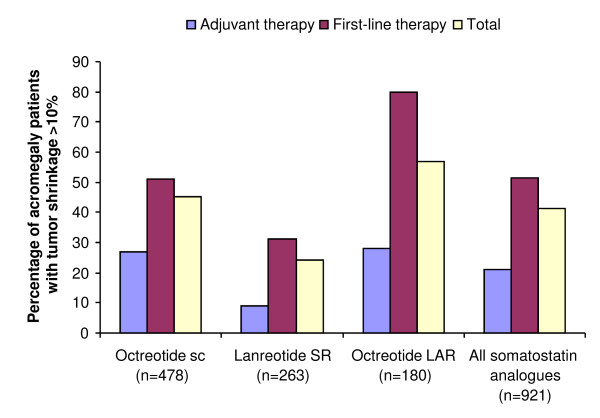
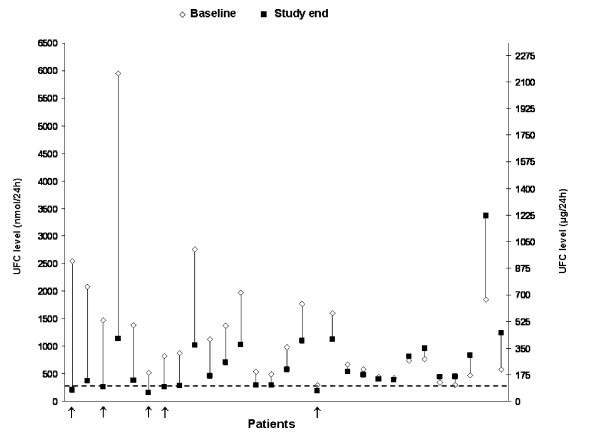
Pituitary adenomas are associated with a variety of clinical manifestations resulting from excessive hormone secretion and tumor mass effects, and require a multidisciplinary management approach. This article discusses the treatment modalities for the management of patients with a prolactinoma, Cushing's disease and acromegaly, and summarizes the options for medical therapy in these patients.First-line treatment of prolactinomas is pharmacotherapy with dopamine agonists; recent reports of cardiac valve abnormalities associated with this class of medication in Parkinson's disease has prompted study in hyperprolactinemic populations. Patients with resistance to dopamine agonists may require other treatment.First-line treatment of Cushing's disease is pituitary surgery by a surgeon with experience in this condition. Current medical options for Cushing's disease block adrenal cortisol production, but do not treat the underlying disease. Pituitary-directed medical therapies are now being explored. In several small studies, the dopamine agonist cabergoline normalized urinary free cortisol in some patients. The multi-receptor targeted somatostatin analogue pasireotide (SOM230) shows promise as a pituitary-directed medical therapy in Cushing's disease; further studies will determine its efficacy and safety. Radiation therapy, with medical adrenal blockade while awaiting the effects of radiation, and bilateral adrenalectomy remain standard treatment options for patients not cured with pituitary surgery.In patients with acromegaly, surgery remains the first-line treatment option when the tumor is likely to be completely resected, or for debulking, especially when the tumor is compressing neurovisual structures. Primary therapy with somatostatin analogues has been used in some patients with large extrasellar tumors not amenable to surgical cure, patients at high surgical risk and patients who decline surgery. Pegvisomant is indicated in patients who have not responded to surgery and other medical therapy, although there are regional differences in when it is prescribed.In conclusion, the treatment of patients with pituitary adenomas requires a multidisciplinary approach. Dopamine agonists are an effective first-line medical therapy in most patients with a prolactinoma, and somatostatin analogues can be used as first-line therapy in selected patients with acromegaly. Current medical therapies for Cushing's disease primarily focus on adrenal blockade of cortisol production, although pasireotide and cabergoline show promise as pituitary-directed medical therapy for Cushing's disease; further long-term evaluation of efficacy and safety is important.
垂体腺瘤与多种临床表现相关,这些临床表现是由于激素分泌过多和肿瘤占位效应引起的,需要采用多学科管理方法。本文讨论了治疗泌乳素瘤、库欣病和肢端肥大症患者的治疗方式,并总结了这些患者的药物治疗选择。
泌乳素瘤的一线治疗方法是多巴胺激动剂药物治疗;最近有报道称,帕金森病患者使用此类药物会导致心脏瓣膜异常,因此对高泌乳素血症患者进行了相关研究。对多巴胺激动剂耐药的患者可能需要其他治疗方法。
库欣病的一线治疗方法是经验丰富的外科医生进行的垂体手术。目前用于库欣病的药物治疗方法是阻断肾上腺皮质醇的产生,但无法治疗潜在疾病。现在正在探索针对垂体的药物治疗方法。在几项小型研究中,多巴胺激动剂卡麦角林使一些患者的尿游离皮质醇恢复正常。多受体靶向生长抑素类似物帕瑞肽(SOM230)作为库欣病的一种针对垂体的药物治疗方法显示出良好的前景;进一步的研究将确定其疗效和安全性。对于未通过垂体手术治愈的患者,在等待放射治疗效果的同时进行药物性肾上腺阻断和双侧肾上腺切除术仍然是标准治疗选择。
对于肢端肥大症患者,当肿瘤有可能完全切除时,手术仍然是一线治疗选择,或者用于肿瘤切除术,尤其是当肿瘤压迫神经视觉结构时。对于大型鞍外肿瘤无法通过手术治愈、手术风险高的患者和拒绝手术的患者,生长抑素类似物可作为一线治疗选择。培维索孟适用于对手术和其他药物治疗无反应的患者,尽管在何时开具该药方面存在区域差异。
总之,垂体腺瘤患者的治疗需要多学科方法。多巴胺激动剂是大多数泌乳素瘤患者有效的一线药物治疗方法,生长抑素类似物可作为特定肢端肥大症患者的一线治疗选择。目前用于库欣病的药物治疗主要侧重于肾上腺皮质醇生成的阻断,尽管帕瑞肽和卡麦角林显示出作为库欣病针对垂体的药物治疗的潜力;进一步评估其疗效和安全性非常重要。