Hospital Clinico Universidad de Chile, Santiago, Chile.
BMC Pediatr. 2010 Jun 3;10:38. doi: 10.1186/1471-2431-10-38.
Respiratory syncytial virus (RSV) is an important pathogen causing annual epidemics of bronchiolitis and pneumonia among infants worldwide. High-risk infants currently receive RSV prophylaxis with palivizumab, a humanized RSV monoclonal antibody (MAb). In preclinical in vitro and in vivo (cotton-rat model) studies, motavizumab, a new RSV MAb, was shown to have greater anti-RSV activity than palivizumab. Motavizumab is currently under review for licensing approval. Since both MAbs may be available concurrently, this study evaluated their safety and tolerability when administered sequentially during the same RSV season.
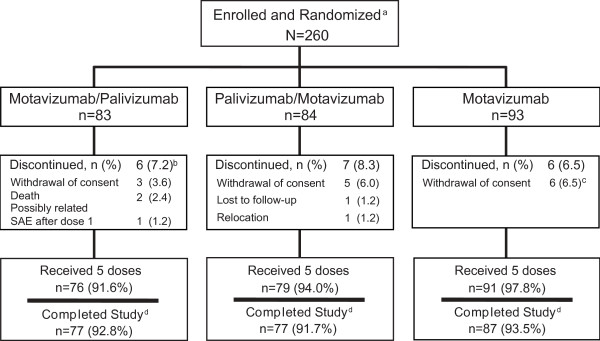
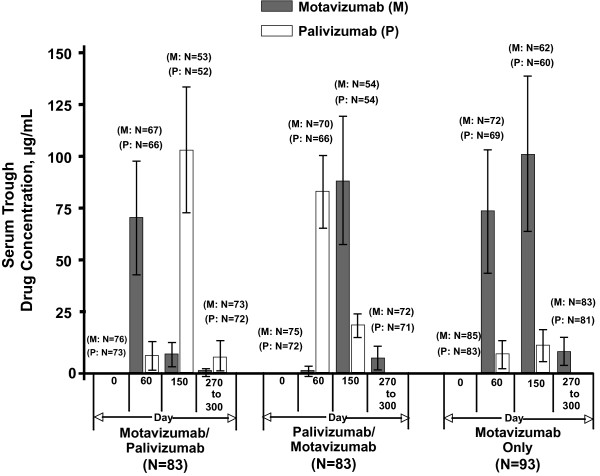
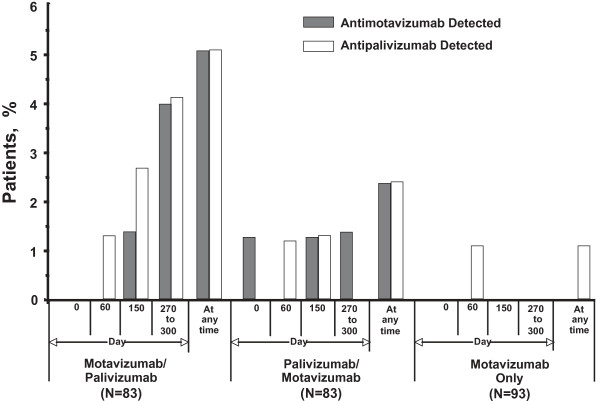
Between April 2006 and May 2006, 260 high-risk infants were randomly assigned 1:1:1 to receive monthly intramuscular injections: 2 doses of motavizumab followed by 3 doses of palivizumab (M/P); 2 doses of palivizumab followed by 3 doses of motavizumab (P/M); or 5 doses of motavizumab (control). Adverse events (AEs, serious AEs [SAEs]), development of antidrug antibody (ADA), and serum drug trough concentrations were assessed.
Most children received all 5 doses (246/260 [94.6%]) and completed the study (241/260 [92.7%]). While overall AE rates were similar (mostly level 1 or 2 in severity), SAEs and level 3 AEs occurred more frequently in the M/P group (SAEs: 22.9% M/P, 8.4% P/M, 11.8% motavizumab only; level 3 AEs: 15.7% M/P, 6.0% P/M, 6.5% motavizumab only). This trend in AE rates occurred before and after switching from motavizumab to palivizumab, suggesting a cause other than the combined regimen. Frequencies of AEs judged by the investigator to be related to study drug were similar among groups. Two deaths occurred on study (both in the M/P group, before palivizumab administration); neither was considered by the site investigator to be related to study drug. Mean serum drug trough concentrations were comparable among groups; ADA detection was infrequent (5.1% or less of any group).
The conclusions drawn from this study are limited by the small sample size per group. However, within this small study, overall AE rates, serum drug trough concentrations, and development of ADA associated with administering motavizumab and palivizumab sequentially to high-risk children appear comparable to administering motavizumab alone during the same RSV season.
clinicaltrials.gov NCT00316264.
呼吸道合胞病毒(RSV)是一种重要的病原体,在全球范围内导致婴儿每年爆发细支气管炎和肺炎。目前,高危婴儿使用帕利珠单抗(一种人源化 RSV 单克隆抗体)进行 RSV 预防。在临床前的体外和体内(棉鼠模型)研究中,莫那比拉珠单抗(一种新的 RSV 单抗)显示出比帕利珠单抗更强的抗 RSV 活性。莫那比拉珠单抗目前正在审查许可批准。由于两种单抗可能同时使用,因此本研究评估了它们在同一 RSV 季节中连续使用时的安全性和耐受性。
2006 年 4 月至 2006 年 5 月,260 名高危婴儿随机 1:1:1 接受每月肌内注射:莫那比拉珠单抗 2 剂,随后帕利珠单抗 3 剂(M/P);帕利珠单抗 2 剂,随后莫那比拉珠单抗 3 剂(P/M);或莫那比拉珠单抗 5 剂(对照)。评估不良事件(AE)、严重不良事件(SAE)、抗药物抗体(ADA)的发展和血清药物谷浓度。
大多数儿童接受了全部 5 剂(260 名中的 246 名[94.6%])并完成了研究(260 名中的 241 名[92.7%])。尽管总体 AE 发生率相似(严重程度大多为 1 级或 2 级),但 M/P 组发生 SAE 和 3 级 AE 的频率更高(SAE:M/P 组 22.9%,P/M 组 8.4%,莫那比拉珠单抗组 11.8%;3 级 AE:M/P 组 15.7%,P/M 组 6.0%,莫那比拉珠单抗组 6.5%)。这种 AE 发生率的趋势在从莫那比拉珠单抗转换为帕利珠单抗之前和之后都出现了,表明这是一种除联合方案以外的原因。各研究组中,研究者判断与研究药物相关的 AE 发生率相似。研究期间发生了 2 例死亡(均在 M/P 组,在帕利珠单抗给药之前);现场研究者均认为与研究药物无关。各组的平均血清药物谷浓度相似;ADA 检测频率较低(任何组均低于 5.1%)。
由于每组的样本量较小,本研究得出的结论受到限制。然而,在这项小型研究中,高危儿童连续使用莫那比拉珠单抗和帕利珠单抗的总体 AE 发生率、血清药物谷浓度和 ADA 发展情况与同一 RSV 季节单独使用莫那比拉珠单抗似乎相似。
clinicaltrials.gov NCT00316264。