Department of Internal Medicine, Gyeongsang National University Hospital, Jinju, Korea.
Korean J Intern Med. 2010 Jun;25(2):154-61. doi: 10.3904/kjim.2010.25.2.154. Epub 2010 Jun 1.
BACKGROUND/AIMS: In patients with coronary artery stents, the cost of clopidogrel has been cited as a factor in the premature discontinuation of therapy. Thus, the introduction of lower-cost generic clopidogrel may increase patient compliance. However, platelet inhibition by generic clopidogrel has not been compared to the original clopidogrel formulation in patients with coronary artery stents.
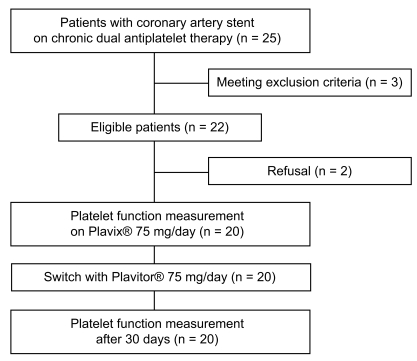
We prospectively enrolled 20 patients receiving chronic therapy with the original clopidogrel bisulfate (Plavix). After assessing patient compliance with Plavix, maintenance therapy was switched to generic clopidogrel bisulfate (Plavitor). Platelet reactivity was assessed at baseline and 30-day after the switch using conventional aggregometry and the VerifyNow P2Y12 assay.
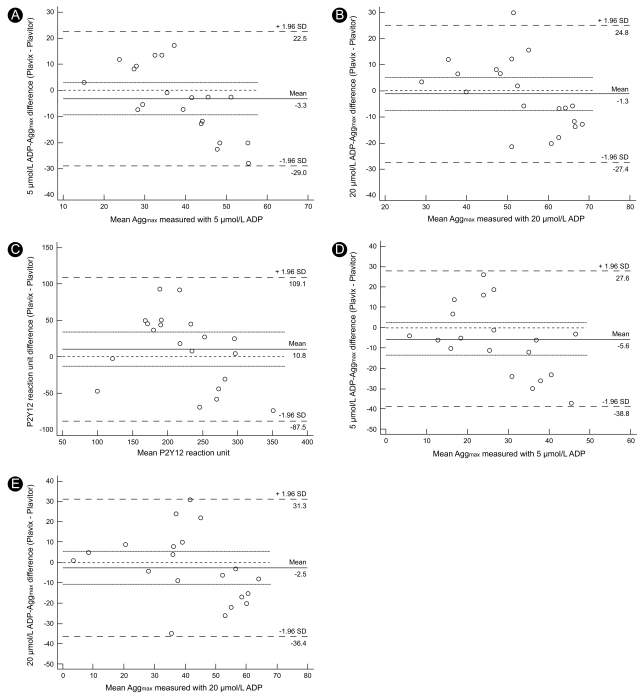
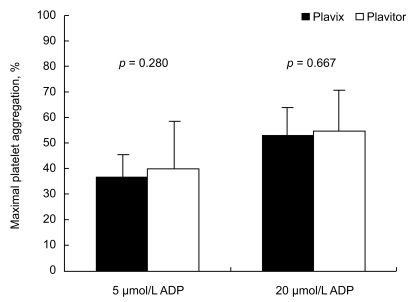
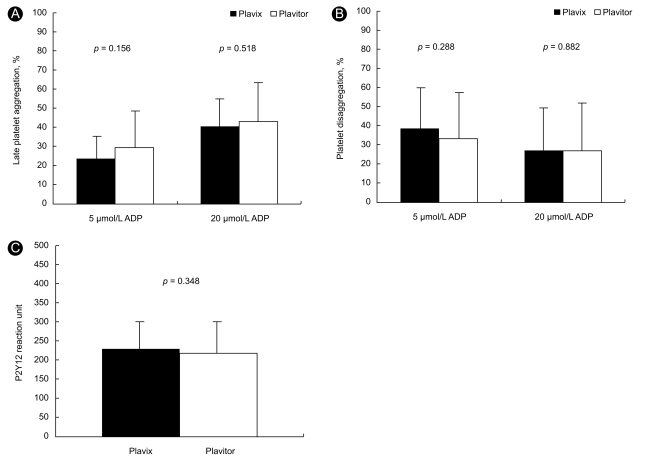
All patients completed maintenance therapy with Plavitor. Before and after switching therapy maximal (36.5 +/- 7.9% vs. 39.8 +/- 16.2%, p = 0.280) and late platelet aggregation (23.5 +/- 10.9% vs. 29.1 +/- 18.3%, p = 0.156) with 5 micromol/L adenosine diphosphate (ADP) stimulus did not differ. Likewise, 20 micromol/L ADP-induced platelet aggregation and P2Y12 reaction unit in patients on Plavitor therapy was comparable to that in patients on Plavix therapy. However, Bland-Altman analysis showed wide limits of agreement between measured platelet reactivity on Plavix vs. Plavitor therapies.
Among patients on Plavix maintenance therapy with coronary stents, replacement with Plavitor shows a comparable inhibition of ADP-induced platelet aggregation. However, due to poor inter-therapy agreement, between two regimens, physicians may be cautious when introducing generic clopidogrel bisulfate.
背景/目的:在接受冠状动脉支架置入术的患者中,氯吡格雷的费用被认为是导致治疗过早中断的一个因素。因此,引入更廉价的仿制药氯吡格雷可能会提高患者的依从性。然而,在接受冠状动脉支架置入术的患者中,尚未比较仿制药氯吡格雷与原研氯吡格雷制剂的血小板抑制作用。
我们前瞻性纳入了 20 例正在接受原研硫酸氢氯吡格雷(波立维)维持治疗的患者。在评估波立维的患者依从性后,将维持治疗方案转换为硫酸氢氯吡格雷(普拉维托)。在转换治疗方案前后,使用常规血小板聚集仪和 VerifyNow P2Y12 检测系统,分别在基线时和 30 天时评估血小板反应性。
所有患者均完成了普拉维托的维持治疗。与治疗前相比,转换治疗方案后最大血小板聚集率(36.5±7.9%比 39.8±16.2%,p=0.280)和晚期血小板聚集率(23.5±10.9%比 29.1±18.3%,p=0.156)用 5μmol/L 二磷酸腺苷(ADP)刺激时无差异。同样,普拉维托治疗患者的 20μmol/L ADP 诱导的血小板聚集率和 P2Y12 反应单位与波立维治疗患者的相似。然而, Bland-Altman 分析显示,波立维与普拉维托治疗方案的血小板反应性之间存在广泛的一致性界限。
在接受冠状动脉支架置入术的接受波立维维持治疗的患者中,用普拉维托替代治疗可达到类似的 ADP 诱导的血小板聚集抑制作用。然而,由于两种方案之间的治疗一致性较差,医生在引入硫酸氢氯吡格雷仿制药时应谨慎。