Department of Medicine, University of Washington, and VA Puget Sound Healthcare System, Seattle, WA 98108, USA.
JAMA. 2010 Jul 14;304(2):180-6. doi: 10.1001/jama.2010.924.
An increasing number of older adults are being treated for end-stage renal disease (ESRD) with long-term dialysis.
To determine how ESRD treatment practices for older adults vary across regions with differing end-of-life intensity of care.
DESIGN, SETTING, AND PARTICIPANTS: Retrospective observational study using a national ESRD registry to identify a cohort of 41,420 adults (of white or black race), aged 65 years or older, who started long-term dialysis or received a kidney transplant between June 1, 2005, and May 31, 2006. Regional end-of-life intensity of care was defined using an index from the Dartmouth Atlas of Healthcare.
Incidence of treated ESRD (dialysis or transplant), preparedness for ESRD (under the care of a nephrologist, having a fistula [vs graft or catheter] at time of hemodialysis initiation), and end-of-life care practices.
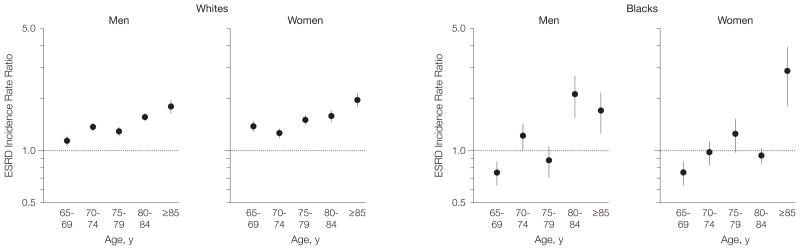
Among whites, the incidence of ESRD was progressively higher in regions with greater intensity of care and this trend was most pronounced at older ages. Among blacks, a similar relationship was present only at advanced ages (men aged > or = 80 years and women aged > or = 85 years). Patients living in regions in the highest compared with lowest quintile of end-of-life intensity of care were less likely to be under the care of a nephrologist before the onset of ESRD (62.3% [95% confidence interval {CI}, 61.3%-63.3%] vs 71.1% [95% CI, 69.9%-72.2%], respectively) and less likely to have a fistula (vs graft or catheter) at the time of hemodialysis initiation (11.2% [95% CI, 10.6%-11.8%] vs 16.9% [95% CI, 15.9%-17.8%]). Among patients who died within 2 years of ESRD onset (n = 21,190), those living in regions in the highest compared with lowest quintile of end-of-life intensity of care were less likely to have discontinued dialysis before death (22.2% [95% CI, 21.1%-23.4%] vs 44.3% [95% CI, 42.5%-46.1%], respectively), less likely to have received hospice care (20.7% [95% CI, 19.5%-21.9%] vs 33.5% [95% CI, 31.7%-35.4%]), and more likely to have died in the hospital (67.8% [95% CI, 66.5%-69.1%] vs 50.3% [95% CI, 48.5%-52.1%]). These differences persisted in adjusted analyses.
There are pronounced regional differences in treatment practices for ESRD in older adults that are not explained by differences in patient characteristics.
越来越多的老年患者接受长期透析治疗终末期肾病(ESRD)。
确定在不同的临终关怀强度地区,老年患者的 ESRD 治疗方法有何不同。
设计、地点和参与者:这是一项使用全国性 ESRD 登记处的回顾性观察性研究,确定了 41420 名年龄在 65 岁或以上的白种人或黑种人(白种或黑种人)成年人队列,他们在 2005 年 6 月 1 日至 2006 年 5 月 31 日期间开始长期透析或接受肾移植。区域临终关怀强度使用达特茅斯医疗保健地图集的指数来定义。
治疗性 ESRD(透析或移植)的发生率、ESRD 治疗准备情况(在肾病学家的护理下,在开始血液透析时具有瘘管[vs 移植物或导管])和临终关怀实践。
在白人中,ESRD 的发病率在临终关怀强度较高的地区逐渐升高,这种趋势在年龄较大时更为明显。在黑人中,只有在高龄时(男性年龄>或=80 岁,女性年龄>或=85 岁)才存在类似的关系。与处于临终关怀强度最低五分位数的地区相比,生活在处于临终关怀强度最高五分位数地区的患者在 ESRD 发病前接受肾病学家护理的可能性较低(62.3%[95%置信区间{CI},61.3%-63.3%]与 71.1%[95% CI,69.9%-72.2%],分别),并且在开始血液透析时更不可能有瘘管(与移植物或导管相比)(11.2%[95% CI,10.6%-11.8%]与 16.9%[95% CI,15.9%-17.8%])。在 ESRD 发病后 2 年内死亡的患者中(n=21190),与处于临终关怀强度最低五分位数的地区相比,处于临终关怀强度最高五分位数的地区的患者在死亡前停止透析的可能性较小(22.2%[95% CI,21.1%-23.4%]与 44.3%[95% CI,42.5%-46.1%],分别),接受临终关怀的可能性较小(20.7%[95% CI,19.5%-21.9%]与 33.5%[95% CI,31.7%-35.4%]),并且更有可能在医院死亡(67.8%[95% CI,66.5%-69.1%]与 50.3%[95% CI,48.5%-52.1%])。这些差异在调整分析中仍然存在。
老年患者的 ESRD 治疗方法存在明显的地区差异,这些差异不能用患者特征的差异来解释。