Division of Nephrology, Department of Medicine, Stanford University School of Medicine, Palo Alto, California.
Geriatric Research and Education Clinical Center, Veterans Affairs (VA) Palo Alto Health Care System, Palo Alto, California.
JAMA Netw Open. 2021 Jan 4;4(1):e2034084. doi: 10.1001/jamanetworkopen.2020.34084.
Current guidelines lack consensus regarding the treatment of patients who may not benefit from dialysis; this lack of consensus may be associated with the substantial variation in dialysis use and outcomes across health care facilities.
To assess the degree to which variation in dialysis use and mortality was associated with patient rather than facility characteristics and to distinguish which features identified the US Department of Veterans Affairs (VA) facilities with high rates of dialysis use.
DESIGN, SETTING, AND PARTICIPANTS: This cohort study analyzed data of veterans with stage 3 or 4 chronic kidney disease that progressed to kidney failure between January 1, 2011, and December 31, 2014. These patients received care from VA facilities across the US. Data sources included laboratory and administrative records from the VA, Medicare, and United States Renal Data System. Data analysis was conducted from August 1, 2019, to September 1, 2020.
The primary exposure was the VA facility in which patients received most of their care before the onset of incident kidney failure defined as the first occurrence of either a sustained estimated glomerular filtration rate of less than 15 mL/min/1.73 m2 or the initiation of maintenance dialysis.
The primary outcomes were dialysis use and mortality within 2 years of incident kidney failure. Median rate ratio was used to quantify facility-level variation, and variance partition coefficient was used to quantify the sources of unexplained variation.
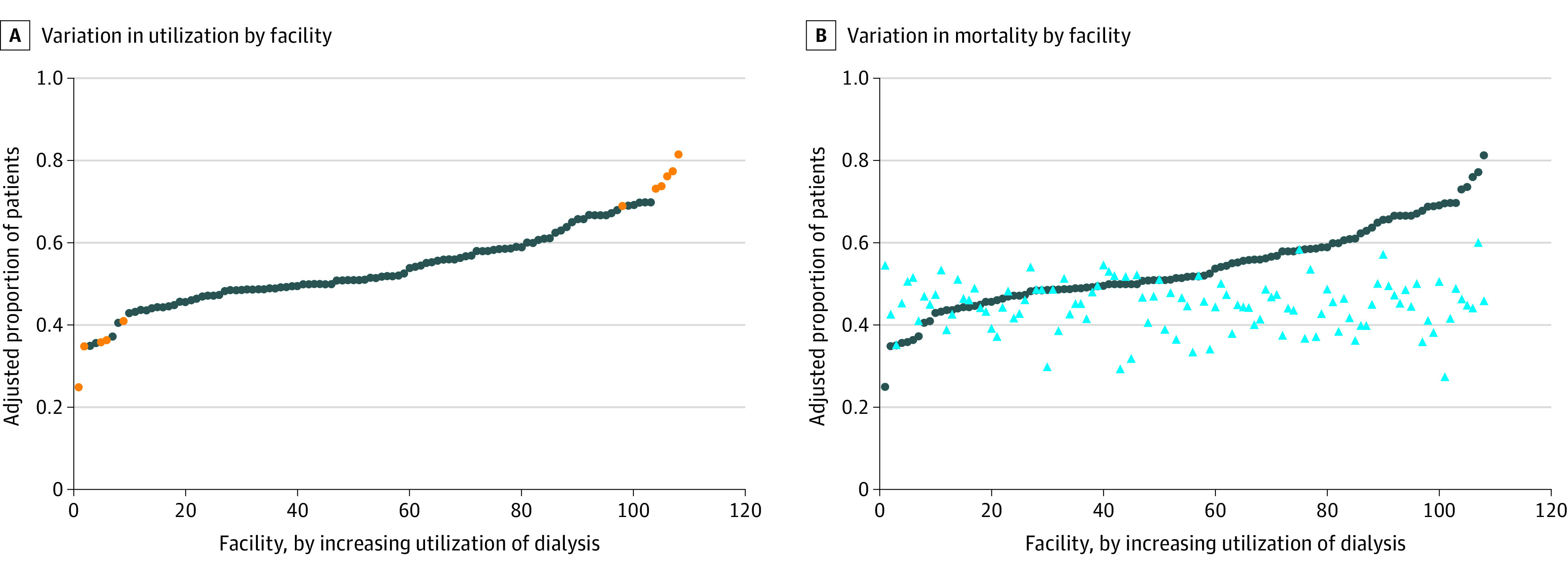
The cohort included 8695 older veterans with a mean (SD) age of 78.8 (7.5) years who were predominantly male (8573 [99%]) and White (6102 [70%]) individuals treated at 108 VA facilities. The observed frequency of dialysis use across facilities ranged from 25.0% to 81.4%, with a median (interquartile range [IQR]) rate of 51.7% (48.4%-60.0%). The observed frequency of mortality across facilities ranged from 27.2% to 60.0%, with a median (IQR) rate of 45.2% (41.2%-48.6%). The median rate ratio (adjusted for multiple patient and facility characteristics) was 1.40 for dialysis use and 1.08 for mortality. The unexplained variation in both outcomes mainly derived from patient characteristics rather than facility characteristics. No correlation was found between dialysis use and mortality at the facility level (correlation coefficient = 0.03).
This study found sizable variation in dialysis use for older adults that was poorly correlated with facility-level mortality rates and was not accounted for by differences in measured patient and facility characteristics. These findings suggest opportunities to improve the degree to which dialysis use practices align with the values, goals, and preferences of older adults with kidney failure.
目前的指南缺乏关于可能无法从透析中获益的患者的治疗共识;这种共识的缺乏可能与医疗机构之间透析使用和结果的巨大差异有关。
评估透析使用和死亡率的变化与患者而不是医疗机构特征的关联程度,并区分哪些特征确定了美国退伍军人事务部(VA)设施具有较高的透析使用率。
设计、设置和参与者:这项队列研究分析了 2011 年 1 月 1 日至 2014 年 12 月 31 日期间因慢性肾脏病 3 或 4 期进展至肾衰竭的退伍军人的数据。这些患者在美国 VA 医疗机构接受治疗。数据来源包括 VA、医疗保险和美国肾脏数据系统的实验室和行政记录。数据分析于 2019 年 8 月 1 日至 2020 年 9 月 1 日进行。
主要暴露是退伍军人在发生肾脏衰竭之前接受大部分治疗的 VA 医疗机构,定义为持续估计肾小球滤过率低于 15 ml/min/1.73 m2或开始维持性透析的首次发生。
主要结局是肾脏衰竭后 2 年内的透析使用和死亡率。中位数率比用于量化医疗机构水平的变异,方差分解系数用于量化未解释变异的来源。
队列包括 8695 名年龄较大的退伍军人,平均(SD)年龄为 78.8(7.5)岁,主要为男性(8573 [99%])和白人(6102 [70%]),在 108 家 VA 医疗机构接受治疗。观察到的设施间透析使用率从 25.0%到 81.4%不等,中位数(四分位距 [IQR])为 51.7%(48.4%-60.0%)。观察到的设施间死亡率从 27.2%到 60.0%不等,中位数(IQR)为 45.2%(41.2%-48.6%)。中位数率比(调整多个患者和医疗机构特征后)为 1.40 用于透析使用,1.08 用于死亡率。两个结果的未解释变异主要来自患者特征,而不是医疗机构特征。在医疗机构水平上未发现透析使用与死亡率之间存在相关性(相关系数=0.03)。
本研究发现,老年人的透析使用存在相当大的差异,与医疗机构的死亡率之间相关性较差,并且不能用测量的患者和医疗机构特征的差异来解释。这些发现表明有机会改善透析使用实践与肾衰竭老年人的价值观、目标和偏好的一致性程度。