Department of Surgery, UCSD Medical Center, 200 West Arbor Drive, San Diego, CA 92103-8999, USA.
J Gastrointest Surg. 2010 Nov;14(11):1782-95. doi: 10.1007/s11605-010-1279-7. Epub 2010 Jul 24.
Emergency treatment of bleeding esophageal varices in cirrhosis is of singular importance because of the high mortality rate. Emergency portacaval shunt is rarely used today because of the belief, unsubstantiated by long-term randomized trials, that it causes frequent portal-systemic encephalopathy and liver failure. Consequently, portacaval shunt has been relegated solely to salvage therapy when endoscopic and pharmacologic therapies have failed.
Is the regimen of endoscopic sclerotherapy with rescue portacaval shunt for failure to control bleeding varices superior to emergency portacaval shunt? A unique opportunity to answer this question was provided by a randomized controlled trial of endoscopic sclerotherapy versus emergency portacaval shunt conducted from 1988 to 2005.
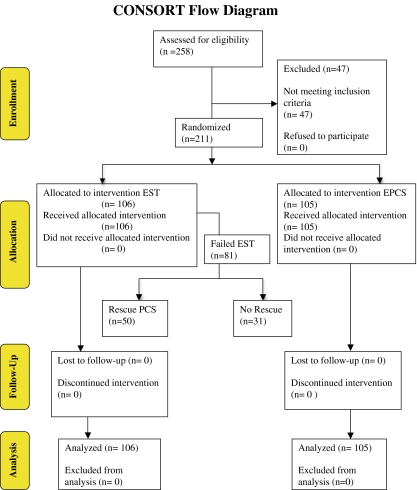
Unselected consecutive cirrhotic patients with acute bleeding esophageal varices were randomized to endoscopic sclerotherapy (n = 106) or emergency portacaval shunt (n = 105). Diagnostic workup was completed and treatment was initiated within 8 h. Failure of endoscopic sclerotherapy was defined by strict criteria and treated by rescue portacaval shunt (n = 50) whenever possible. Ninety-six percent of patients had more than 10 years of follow-up or until death.
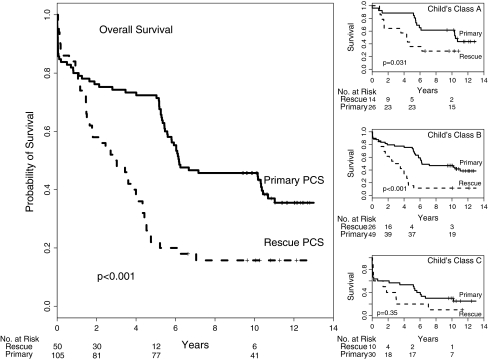
Comparison of emergency portacaval shunt and endoscopic sclerotherapy followed by rescue portacaval shunt showed the following differences in measurements of outcomes: (1) survival after 5 years (72% versus 22%), 10 years (46% versus 16%), and 15 years (46% versus 0%); (2) median post-shunt survival (6.18 versus 1.99 years); (3) mean requirements of packed red blood cell units (17.85 versus 27.80); (4) incidence of recurrent portal-systemic encephalopathy (15% versus 43%); (5) 5-year change in Child's class showing improvement (59% versus 19%) or worsening (8% versus 44%); (6) mean quality of life points in which lower is better (13.89 versus 27.89); and (7) mean cost of care per year ($39,200 versus $216,700). These differences were highly significant in favor of emergency portacaval shunt (all p < 0.001).
Emergency portacaval shunt was strikingly superior to endoscopic sclerotherapy as well as to the combination of endoscopic sclerotherapy and rescue portacaval shunt in regard to all outcome measures, specifically bleeding control, survival, incidence of portal-systemic encephalopathy, improvement in liver function, quality of life, and cost of care. These results strongly support the use of emergency portacaval shunt as the first line of emergency treatment of bleeding esophageal varices in cirrhosis.
由于肝硬化导致的食管静脉曲张出血的死亡率很高,因此对其进行紧急治疗具有重要意义。由于缺乏长期随机试验的支持,人们普遍认为急诊门腔分流术会导致频繁的门体系统脑病和肝功能衰竭,因此目前很少使用。因此,只有在内镜和药物治疗失败时,才将门腔分流术用于挽救治疗。
内镜硬化治疗加紧急门腔分流术治疗静脉曲张出血控制失败是否优于紧急门腔分流术?一项独特的机会回答了这个问题,即 1988 年至 2005 年期间进行的内镜硬化治疗与紧急门腔分流术的随机对照试验。
未经选择的连续患有急性食管静脉曲张出血的肝硬化患者被随机分为内镜硬化治疗组(n=106)或紧急门腔分流术组(n=105)。在 8 小时内完成诊断性检查并开始治疗。内镜硬化治疗失败的定义为严格标准,并在可能的情况下通过紧急门腔分流术进行治疗(n=50)。96%的患者随访超过 10 年或直至死亡。
比较紧急门腔分流术和内镜硬化治疗加紧急门腔分流术治疗后发现,以下结果测量指标存在差异:(1)5 年生存率(72%比 22%)、10 年生存率(46%比 16%)和 15 年生存率(46%比 0%);(2)分流术后中位生存时间(6.18 比 1.99 年);(3)平均需要的浓缩红细胞单位(17.85 比 27.80);(4)复发性门体系统脑病的发生率(15%比 43%);(5)Child 分级 5 年变化显示改善(59%比 19%)或恶化(8%比 44%);(6)生活质量评分(分数越低越好),13.89 比 27.89;(7)每年护理费用(39200 美元比 216700 美元)。这些差异均具有统计学意义,紧急门腔分流术具有显著优势(均 p<0.001)。
紧急门腔分流术在所有结果测量指标上,尤其是在出血控制、生存率、门体系统脑病发生率、肝功能改善、生活质量和护理费用方面,均显著优于内镜硬化治疗以及内镜硬化治疗加紧急门腔分流术。这些结果强烈支持将紧急门腔分流术作为肝硬化食管静脉曲张出血的一线急救治疗方法。