Department of Physical Therapy, University of Florida, Gainesville, FL 32611, USA.
J Pain. 2011 Jan;12(1):133-40. doi: 10.1016/j.jpain.2010.06.002. Epub 2010 Aug 7.
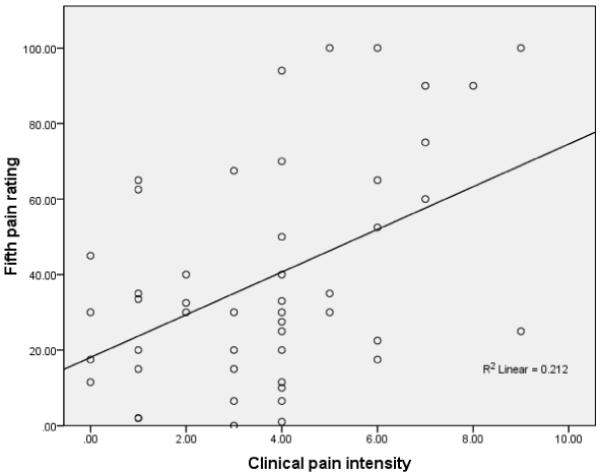
Quantitative sensory testing (QST) has become commonly used for the assessment of pain in subjects with clinical conditions. However, there is no consensus about which type of QST is the best predictor of clinical pain responses. The purposes of this study were to determine: a) the QST measure with the strongest association with clinical pain intensity; and b) if the QST measure continued to predict clinical pain intensity in a model including relevant psychological factors. Fifty-nine patients seeking treatment for shoulder pain underwent experimental pain assessment involving heat and pressure stimuli. The patients also completed validated questionnaires for pain intensity, pain catastrophizing, anxiety, and depression. The 5th pain rating in a series of suprathreshold heat pain stimuli accounted for a significant amount of variance in clinical pain intensity, with no other QST measure contributing to the model. The 5th pain rating remained a significant contributor to clinical pain intensity when psychological factors were included in the model. Furthermore, subjects with elevated 5th pain rating, pain catastrophizing, and depression scores had higher clinical pain intensity ratings in pre- and postoperative assessments. These data suggest that assessment of pain should include suprathreshold heat stimuli and psychological factors separately, and a combination of these factors may be predictive of pain intensity outcomes.
The current study provides evidence for a suprathreshold heat pain response as a clinically relevant QST measure for patients with shoulder pain, even after psychological factors were considered. The present findings suggest that the 5th pain rating from a series of suprathreshold stimuli, pain catastrophizing, and depression might play a role in predicting pain intensity outcomes.
定量感觉测试(QST)已广泛用于评估有临床症状的受试者的疼痛。然而,哪种 QST 是临床疼痛反应的最佳预测指标尚未达成共识。本研究的目的是确定:a)与临床疼痛强度关联最强的 QST 测量方法;b)如果 QST 测量方法在包括相关心理因素的模型中是否继续预测临床疼痛强度。59 名寻求肩部疼痛治疗的患者接受了涉及热和压力刺激的实验性疼痛评估。患者还完成了疼痛强度、疼痛灾难化、焦虑和抑郁的有效问卷。一系列超阈值热痛刺激中的第 5 次疼痛评分解释了临床疼痛强度的大量差异,没有其他 QST 测量方法对模型有贡献。当将心理因素纳入模型时,第 5 次疼痛评分仍然是临床疼痛强度的重要贡献者。此外,第 5 次疼痛评分、疼痛灾难化和抑郁评分较高的患者在术前和术后评估中的临床疼痛强度评分更高。这些数据表明,疼痛评估应分别包括超阈值热刺激和心理因素,这些因素的组合可能预测疼痛强度结果。
本研究为肩部疼痛患者的超阈值热痛反应提供了作为临床相关 QST 测量的证据,即使考虑了心理因素也是如此。目前的研究结果表明,一系列超阈值刺激中的第 5 次疼痛评分、疼痛灾难化和抑郁可能在预测疼痛强度结果方面发挥作用。