Cheon Jaewoo, Chung Hyunchul, Song Jaemann
Department of Urology, Wonju Christian Hospital, Wonju Yonsei College of Medicine, Wonju, Korea.
Korean J Urol. 2010 Aug;51(8):525-30. doi: 10.4111/kju.2010.51.8.525. Epub 2010 Aug 18.
Radical cystectomy has been the most widely used method in the treatment of bladder cancer, but it is limited by major problems. Therefore, we investigated the results of bladder-preserving treatment in patients with T3b, T4a, and T4b transitional carcinoma of the bladder who underwent transurethral resection of bladder cancer and subsequent administration of chemotherapy.
Of all patients who were diagnosed with bladder cancer and underwent bladder-preserving treatment between January 2001 and August 2008, 78 patients with at least 12 months of follow-up data were enrolled in this study. All patients received gemcitabine (1,000 mg/m(2)) and cisplatin (70 mg/m(2)) once per month postoperatively for a total of 6 months and completed a follow-up visit every 3 months. The patient survival rate and prognostic factors (age, tumor size, differentiation, number of lesions, stage, and presence of hydronephrosis) were assessed. The Kaplan-Meier method was used to analyze survival rate, and Cox multiple regression analysis was used for prognostic factors.
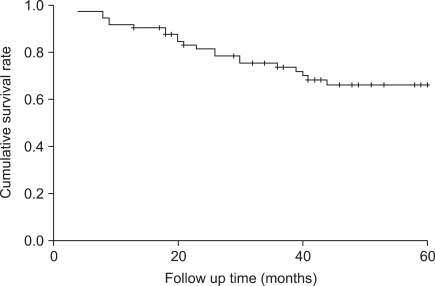
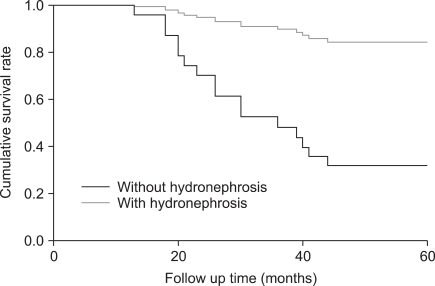
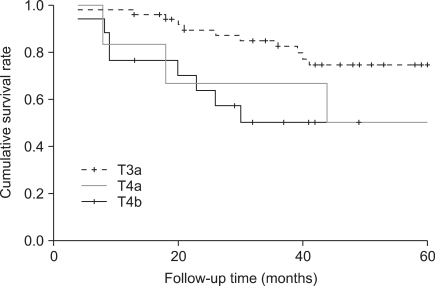
The mean patient age was 68.32+/-8.6 years, the mean duration of follow-up was 54.70+/-32.8 months, and the median duration of follow-up was 49.0 months. The 5-year survival rate was 66.2%. Single lesions were found in 28 cases (35.9%), and multiple lesions were found in 50 cases (64.1%). Stage T3b lesions were identified in 56 cases (71.8%), stage T4a lesions were identified in 16 cases (20.5%), and stage T4b lesions were identified in 6 cases (7.7%). Tumor size was less than 4 cm in 4 cases (59.0%) and greater than 4 cm in 32 (41.0%). Hydronephrosis was present in 21 cases (26.9%). In the 5-year survival analysis, prognostic factors significantly influencing survival rate were T-stage of the tumor and absence of hydronephrosis and complete regression after treatment (p<0.05). Multivariate analysis revealed that tumor stage and the absence of hydronephrosis were statistically significant prognostic indicators.
In patients with T3b, T4a, and T4b transitional carcinoma of the bladder, bladder preservation may prevent a decrease in quality of life. Also, our findings suggest that this approach could be considered a primary treatment option for patients with T3b stage tumors without evidence of hydronephrosis.
根治性膀胱切除术一直是治疗膀胱癌最广泛使用的方法,但它受到一些主要问题的限制。因此,我们研究了经尿道膀胱癌切除术并随后进行化疗的T3b、T4a和T4b期膀胱移行癌患者的保膀胱治疗结果。
在2001年1月至2008年8月期间被诊断为膀胱癌并接受保膀胱治疗的所有患者中,78例有至少12个月随访数据的患者被纳入本研究。所有患者术后每月接受一次吉西他滨(1000mg/m²)和顺铂(70mg/m²),共6个月,并每3个月进行一次随访。评估患者生存率和预后因素(年龄、肿瘤大小、分化程度、病变数量、分期和肾积水情况)。采用Kaplan-Meier法分析生存率,采用Cox多元回归分析预后因素。
患者平均年龄为68.32±8.6岁,平均随访时间为54.70±32.8个月,中位随访时间为49.0个月。5年生存率为66.2%。28例(35.9%)发现单个病变,50例(64.1%)发现多个病变。56例(71.8%)为T3b期病变,16例(20.5%)为T4a期病变,6例(7.7%)为T4b期病变。4例(59.0%)肿瘤大小小于4cm,32例(41.0%)大于4cm。21例(26.9%)存在肾积水。在5年生存分析中,显著影响生存率的预后因素是肿瘤的T分期、无肾积水以及治疗后完全缓解(p<0.05)。多变量分析显示肿瘤分期和无肾积水是具有统计学意义的预后指标。
对于T3b、T4a和T4b期膀胱移行癌患者,保膀胱治疗可能预防生活质量下降。此外,我们的研究结果表明,对于无肾积水证据的T3b期肿瘤患者,这种方法可被视为一种主要治疗选择。