Eli Lilly and Company, Indianapolis, IN USA.
BMC Psychiatry. 2010 Sep 28;10:75. doi: 10.1186/1471-244X-10-75.
To identify patient characteristics and early changes in patients' clinical status that best predict subsequent switching of antipsychotic agents in the long-term treatment of schizophrenia.
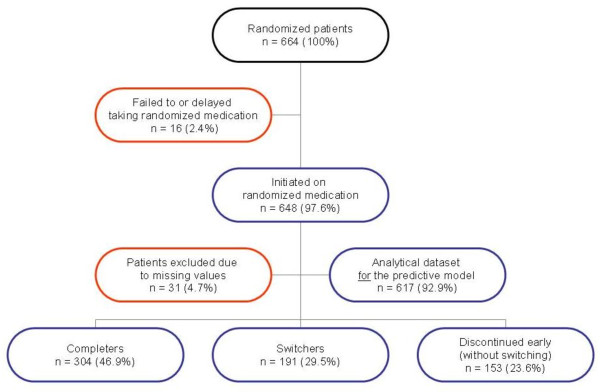
This post-hoc analysis used data from a one-year randomized, open-label, multisite study of antipsychotics in the treatment of schizophrenia. The study protocol permitted switching of antipsychotics when clinically warranted after the first eight weeks. Baseline patient characteristics were assessed using standard psychiatric measures and reviews of medical records. The prediction model included baseline sociodemographics, comorbid psychiatric and non-psychiatric conditions, body weight, clinical and functional variables, as well as change scores on standard efficacy and tolerability measures during the first two weeks of treatment. Cox proportional hazards modeling was used to identify the best predictors of switching from the initially assigned antipsychotic medication.
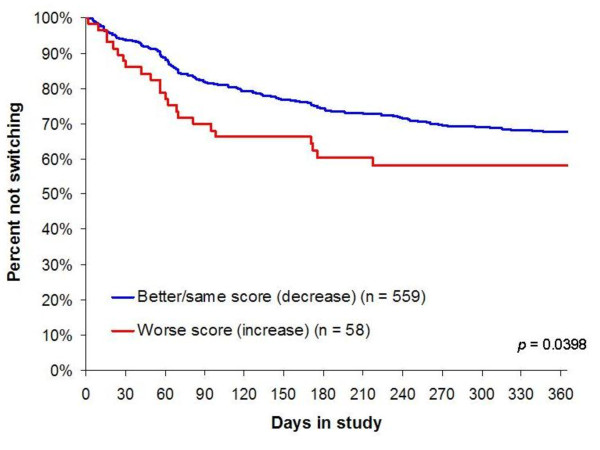
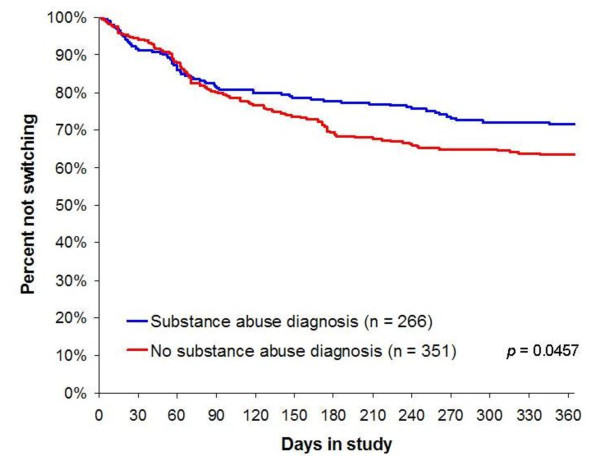
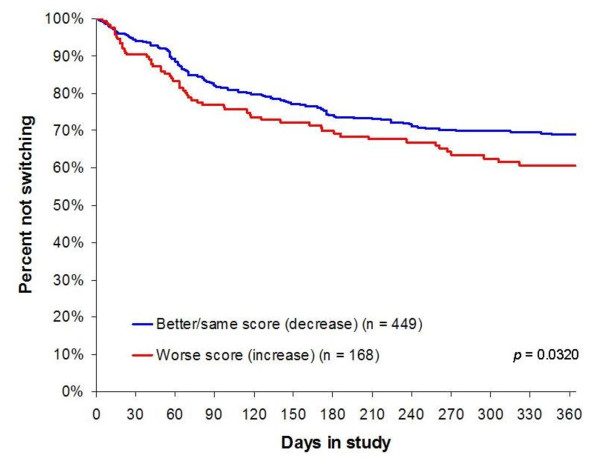
About one-third of patients (29.5%, 191/648) switched antipsychotics before the end of the one-year study. There were six variables identified as the best predictors of switching: lack of antipsychotic use in the prior year, pre-existing depression, female gender, lack of substance use disorder, worsening of akathisia (as measured by the Barnes Akathisia Scale), and worsening of symptoms of depression/anxiety (subscale score on the Positive and Negative Syndrome Scale) during the first two weeks of antipsychotic therapy.
Switching antipsychotics appears to be prevalent in the naturalistic treatment of schizophrenia and can be predicted by a small and distinct set of variables. Interestingly, worsening of anxiety and depressive symptoms and of akathisia following two weeks of treatment were among the more robust predictors of subsequent switching of antipsychotics.
确定能够预测精神分裂症长期治疗中抗精神病药物后续转换的患者特征和临床状态早期变化。
这项回顾性分析使用了为期一年的、针对精神分裂症的抗精神病药物开放标签、随机、多中心治疗研究的数据。该研究方案规定,在最初的八周后,如果临床需要,可以更换抗精神病药物。使用标准精神科评估和病历回顾来评估患者的基线特征。预测模型包括基线人口统计学、合并的精神和非精神疾病、体重、临床和功能变量,以及治疗的前两周内标准疗效和耐受性测量的变化分数。使用 Cox 比例风险模型来确定从最初分配的抗精神病药物转换的最佳预测因子。
大约三分之一的患者(29.5%,191/648)在一年研究结束前更换了抗精神病药物。有六个变量被确定为转换的最佳预测因子:前一年没有使用抗精神病药物、预先存在的抑郁症、女性、没有物质使用障碍、静坐不能恶化(用巴恩斯静坐不能量表测量)和治疗的前两周内抑郁/焦虑症状恶化(阳性和阴性综合征量表的子量表评分)。
在精神分裂症的自然治疗中,更换抗精神病药物似乎很常见,可以通过一小部分独特的变量来预测。有趣的是,治疗两周后焦虑和抑郁症状以及静坐不能的恶化是后续抗精神病药物转换的更有力预测因子之一。