Department of Blood and Marrow Transplantation, Moffitt Cancer Center, 12902 Magnolia Drive, Tampa, FL 33612, USA.
J Hematol Oncol. 2010 Oct 6;3:36. doi: 10.1186/1756-8722-3-36.
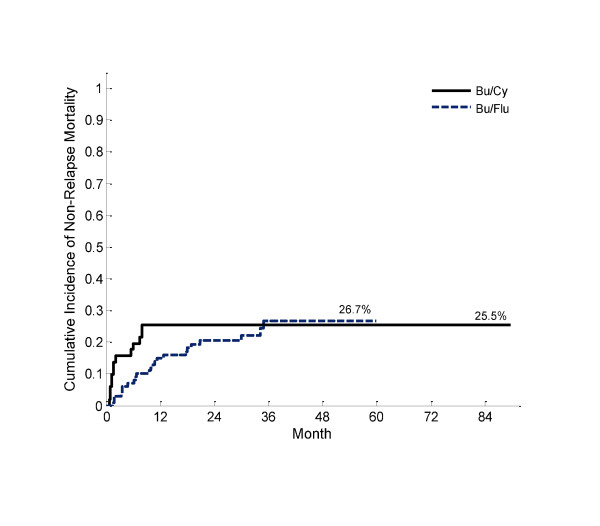
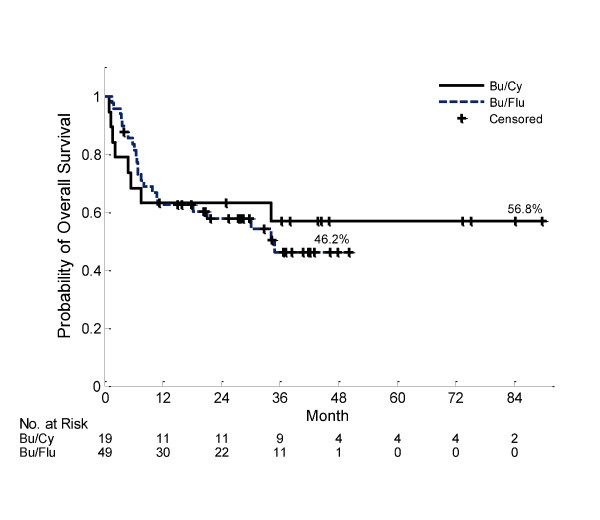
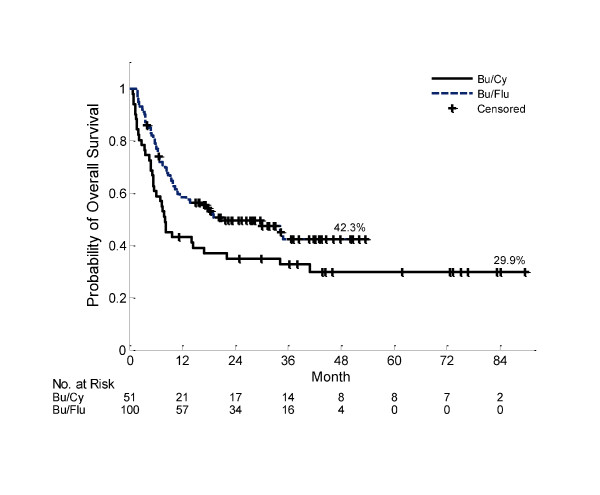
Optimal conditioning therapy for hematopoietic cell transplantation (HCT) in acute myelogenous leukemia (AML) remains undefined. We retrospectively compared outcomes of a consecutive series of 51 AML patients treated with oral busulfan (1 mg/kg every 6 hours for 4 days) and cyclophosphamide (60 mg/kg IV × 2 days) - (Bu/Cy) with 100 consecutive AML patients treated with pharmacokinetic targeted IV busulfan (AUC < 6000 μM/L*min per day × 4 days) and fludarabine (40 mg/m2 × 4 days) - (t-IV Bu/Flu). The Bu/Cy and t-IV Bu/Flu groups significantly differed according to donor relation, stem cell source, aGVHD prophylaxis, remission status, primary vs. secondary disease, median age, and % blasts prior to HCT (p < 0.01 for each). Conditioning with t-IV Bu/Flu reduced early toxicity including idiopathic pneumonia syndrome (IPS) and hepatic veno-occlusive disease (VOD). Additionally, the trajectory of early NRM (100 day: 16% vs. 3%, and1 year: 25% vs. 15% for Bu/Cy and t-IV Bu/Flu, respectively) favored t-IV Bu/Flu. Grade II-IV aGVHD (48% vs. 82%, p < 0.0001), as well as moderate/severe cGVHD (7% vs. 40%, p < 0.0001) differed between the Bu/Cy and t-IV Bu/Flu groups, due to the predominance of peripheral blood stem cells in the t-IV Bu/Flu group. Pharmacokinetic targeting of intravenous busulfan in combination with fludarabine is associated with reduced conditioning regimen related toxicity compared to oral busulfan and cyclophosphamide. However, multivariable analysis did not demonstrate significant differences in overall survival (p = 0.78) or non-relapse mortality (p = 0.6) according to conditioning regimen delivered.
异基因造血细胞移植(HCT)治疗急性髓系白血病(AML)的最佳预处理方案仍不明确。我们回顾性比较了连续 51 例 AML 患者接受口服白消安(1mg/kg,每 6 小时 1 次,连用 4 天)和环磷酰胺(60mg/kg,静脉滴注 2 天)预处理方案(Bu/Cy)与 100 例连续 AML 患者接受药代动力学靶向静脉白消安(AUC<6000μM/L*min/天×4 天)和氟达拉滨(40mg/m2×4 天)预处理方案(t-IV Bu/Flu)的治疗结果。Bu/Cy 和 t-IV Bu/Flu 两组患者在供者关系、干细胞来源、急性移植物抗宿主病(aGVHD)预防、缓解状态、初治/复发疾病、中位年龄和 HCT 前原始细胞比例等方面差异显著(p<0.01)。与 Bu/Cy 相比,t-IV Bu/Flu 预处理降低了早期毒性,包括特发性肺炎综合征(IPS)和肝静脉闭塞性疾病(VOD)。此外,早期非复发死亡率(100 天:16%比 3%,1 年:25%比 15%,Bu/Cy 和 t-IV Bu/Flu 组)也有利于 t-IV Bu/Flu。Ⅱ-Ⅳ级 aGVHD(48%比 82%,p<0.0001)和中重度慢性移植物抗宿主病(cGVHD)(7%比 40%,p<0.0001)也在 Bu/Cy 和 t-IV Bu/Flu 两组间存在差异,这是由于 t-IV Bu/Flu 组以外周血干细胞为主。与口服白消安和环磷酰胺相比,静脉白消安联合氟达拉滨的药代动力学靶向治疗与预处理相关毒性降低有关。然而,多变量分析显示,根据预处理方案的不同,总生存(p=0.78)或非复发死亡率(p=0.6)无显著差异。