Sayed-Ahmed Mohamed M, Darweesh Amal Q, Fatani Amal J
Department of Pharmacology; College of Pharmacy; King Saud University; Riyadh, Kingdom of Saudi Arabia.
Oxid Med Cell Longev. 2010 Jul-Aug;3(4):266-74. doi: 10.4161/oxim.3.4.12859.
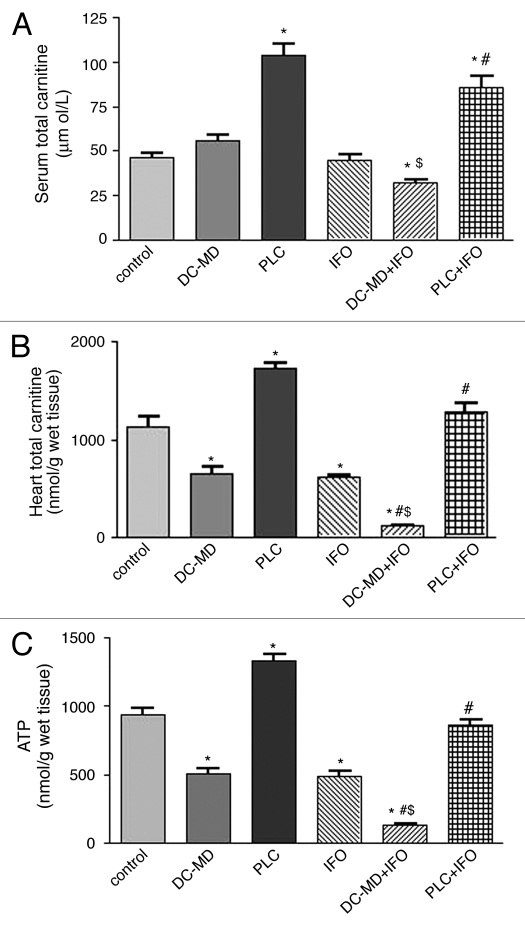
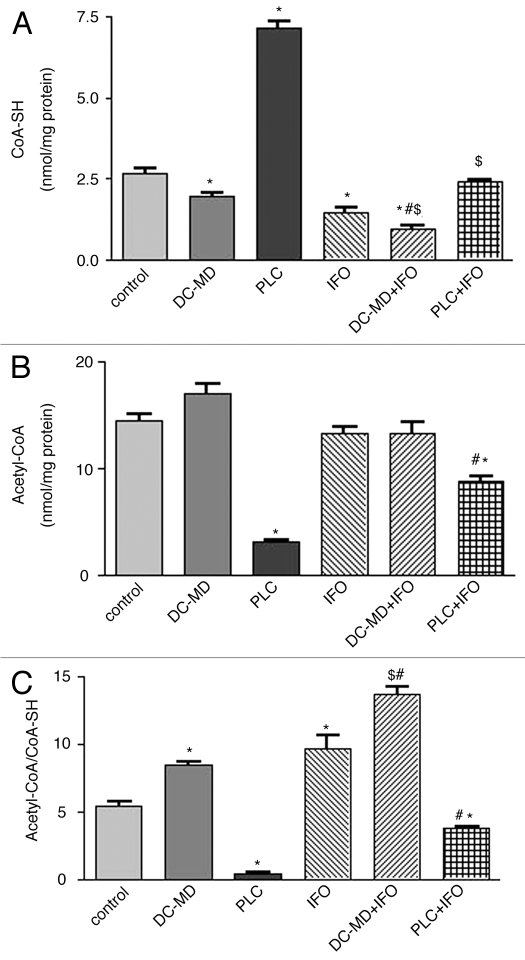
In addition to hemorrhagic cystitis, Fanconi Syndrome is a serious clinical side effect during ifosfamide (IFO) therapy. Fanconi syndrome is a generalized dysfunction of the proximal tubule which is characterized by excessive urinary excretion of glucose, phosphate, bicarbonate, amino acids and other solutes excreted by this segment of the nephron including L-carnitine. Carnitine is essential cofactor for β-oxidation of long-chain fatty acids in the myocardium. IFO therapy is associated with increased urinary carnitine excretion with subsequent secondary deficiency of the molecule. Cardiac abnormalities in IFO-treated cancer patients were reported as isolated clinical cases. This study examined whether carnitine deficiency and oxidative stress, secondary to Fanconi Syndrome, provoke IFO-induced cardiomyopathy as well as exploring if carnitine supplementation using Propionyl-L-carnitine (PLC) could offer protection against this toxicity. In the current study, an animal model of carnitine deficiency was developed in rats by D-carnitine-mildronate treatment Adult male Wistar albino rats were assigned to one of six treatment groups: the first three groups were injected intraperitoneally with normal saline, D-carnitine (DC, 250 mg/kg/day) combined with mildronate (MD, 200 mg/kg/day) and PLC (250 mg/kg/day), respectively, for 10 successive days. The 4(th), 5(th) and 6(th) groups were injected with the same doses of normal saline, DC-MD and PLC, respectively for 5 successive days before and 5 days concomitant with IFO (50 mg/kg/day). IFO significantly increased serum creatinine, blood urea nitrogen (BUN), urinary carnitine excretion and clearance, creatine phosphokinase isoenzyme (CK-MB), lactate dehydrogenase (LDH), intramitochondrial acetyl-CoA/CoA-SH and thiobarbituric acid reactive substances (TBARS) in cardiac tissues and significantly decreased adenosine triphosphate (ATP) and total carnitine and reduced glutathione (GSH) content in cardiac tissues. In carnitine-depleted rats, IFO induced dramatic increase in serum creatinine, BUN, CK-MB, LDH, carnitine clearance and intramitochondrial acetyl-CoA/CoA-SH, as well as progressive reduction in total carnitine and ATP in cardiac tissues. Interestingly, PLC supplementation completely reversed the biochemical changes-induced by IFO to the control values. In conclusion, data from the present study suggest that: Carnitine deficiency and oxidative stress, secondary to Fanconi Syndrome, constitute risk factors and should be viewed as mechanisms during development of IFO-induced cardiotoxicity. Carnitine supplementation, using PLC, prevents the development of IFO-induced cardiotoxicity through antioxidant signalling and improving mitochondrial function.
除出血性膀胱炎外,范科尼综合征是异环磷酰胺(IFO)治疗期间严重的临床副作用。范科尼综合征是近端小管的广泛性功能障碍,其特征是葡萄糖、磷酸盐、碳酸氢盐、氨基酸以及肾单位该节段排泄的其他溶质(包括左旋肉碱)过度经尿排泄。肉碱是心肌中长链脂肪酸β氧化的必需辅助因子。IFO治疗与尿肉碱排泄增加以及随后该分子的继发性缺乏有关。IFO治疗的癌症患者出现心脏异常的情况曾有个别临床病例报道。本研究考察了继发于范科尼综合征的肉碱缺乏和氧化应激是否会引发IFO诱导的心肌病,以及探索使用丙酰左旋肉碱(PLC)补充肉碱是否能预防这种毒性。在本研究中,通过D - 肉碱 - 米屈肼处理在大鼠中建立了肉碱缺乏的动物模型。成年雄性Wistar白化大鼠被分配到六个治疗组之一:前三组分别连续10天腹腔注射生理盐水、D - 肉碱(DC,250 mg/kg/天)联合米屈肼(MD,200 mg/kg/天)和PLC(250 mg/kg/天)。第4、5和6组在IFO(50 mg/kg/天)给药前连续5天以及给药期间连续5天分别注射相同剂量的生理盐水、DC - MD和PLC。IFO显著增加血清肌酐、血尿素氮(BUN)、尿肉碱排泄和清除率、肌酸磷酸激酶同工酶(CK - MB)、乳酸脱氢酶(LDH)、心脏组织线粒体内乙酰辅酶A/辅酶A - SH和硫代巴比妥酸反应性物质(TBARS),并显著降低心脏组织中的三磷酸腺苷(ATP)、总肉碱和还原型谷胱甘肽(GSH)含量。在肉碱缺乏的大鼠中,IFO导致血清肌酐、BUN、CK - MB、LDH、肉碱清除率和线粒体内乙酰辅酶A/辅酶A - SH显著增加,以及心脏组织中总肉碱和ATP逐渐减少。有趣的是,补充PLC可使IFO诱导的生化变化完全恢复至对照值。总之,本研究数据表明:继发于范科尼综合征的肉碱缺乏和氧化应激构成风险因素,应被视为IFO诱导的心脏毒性发生过程中的机制。使用PLC补充肉碱可通过抗氧化信号传导和改善线粒体功能预防IFO诱导的心脏毒性。