Department of Medicine, University of Colorado Denver, Aurora, USA.
Diabetes. 2011 Jan;60(1):306-14. doi: 10.2337/db10-0328. Epub 2010 Oct 26.
To assess insulin action on peripheral glucose utilization and nonesterified fatty acid (NEFA) suppression as a predictor of coronary artery calcification (CAC) in patients with type 1 diabetes and nondiabetic controls.
Insulin action was measured by a three-stage hyperinsulinemic-euglycemic clamp (4, 8, and 40 mU/m²/min) in 87 subjects from the Coronary Artery Calcification in Type 1 Diabetes cohort (40 diabetic, 47 nondiabetic; mean age 45 ± 8 years; 55% female).
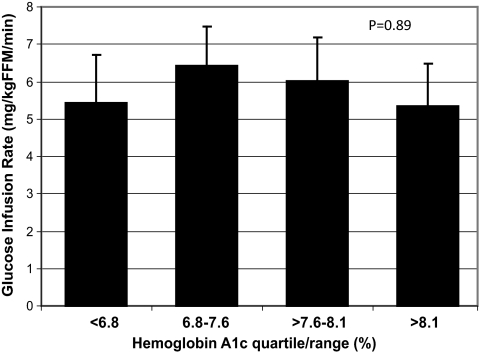
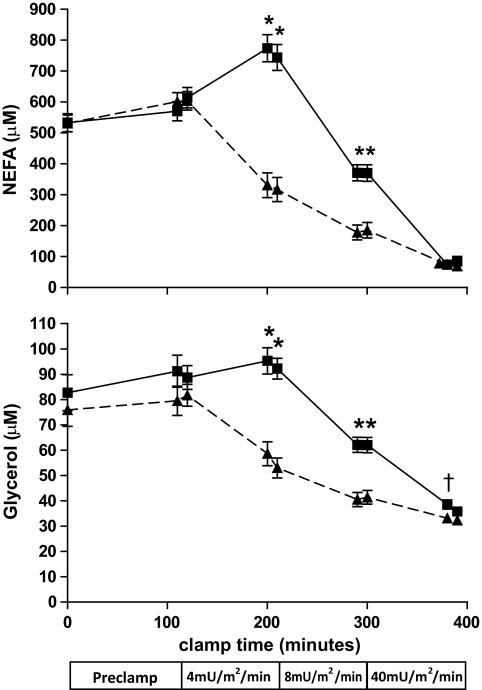
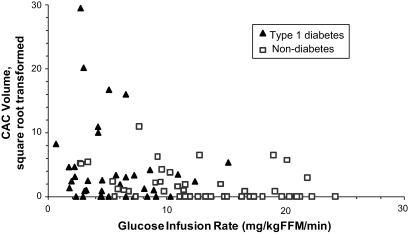
Peripheral glucose utilization was lower in subjects with type 1 diabetes compared with nondiabetic controls: glucose infusion rate (mg/kg FFM/min) = 6.19 ± 0.72 vs. 12.71 ± 0.66, mean ± SE, P < 0.0001, after adjustment for age, sex, BMI, fasting glucose, and final clamp glucose and insulin. Insulin-induced NEFA suppression was also lower in type 1 diabetic compared with nondiabetic subjects: NEFA levels (μM) during 8 mU/m²/min insulin infusion = 370 ± 27 vs. 185 ± 25, P < 0.0001, after adjustment for age, sex, BMI, fasting glucose, and time point insulin. Lower glucose utilization and higher NEFA levels, correlated with CAC volume (r = -0.42, P < 0.0001 and r = 0.41, P < 0.0001, respectively) and predicted the presence of CAC (odds ratio [OR] = 0.45, 95% CI = 0.22-0.93, P = 0.03; OR = 2.4, 95% CI = 1.08-5.32, P = 0.032, respectively). Insulin resistance did not correlate with GHb or continuous glucose monitoring parameters.
Type 1 diabetic patients are insulin resistant compared with nondiabetic subjects, and the degree of resistance is not related to current glycemic control. Insulin resistance predicts the extent of coronary artery calcification and may contribute to the increased risk of cardiovascular disease in patients with type 1 diabetes as well as subjects without diabetes.
评估胰岛素对周围葡萄糖利用和非酯化脂肪酸(NEFA)抑制的作用,作为 1 型糖尿病患者和非糖尿病对照者冠状动脉钙化(CAC)的预测因子。
在 1 型糖尿病冠状动脉钙化队列(40 例糖尿病,47 例非糖尿病;平均年龄 45 ± 8 岁;55%为女性)的 87 名受试者中,通过三阶段高胰岛素-正葡萄糖钳夹(4、8 和 40 mU/m²/min)测量胰岛素作用。
与非糖尿病对照组相比,1 型糖尿病患者的外周葡萄糖利用率较低:葡萄糖输注率(mg/kg FFM/min)= 6.19 ± 0.72 与 12.71 ± 0.66,平均值 ± SE,P < 0.0001,调整年龄、性别、BMI、空腹血糖和最终钳夹葡萄糖和胰岛素后。与非糖尿病受试者相比,1 型糖尿病患者的胰岛素诱导的 NEFA 抑制作用也较低:8 mU/m²/min 胰岛素输注时的 NEFA 水平(μM)= 370 ± 27 与 185 ± 25,P < 0.0001,调整年龄、性别、BMI、空腹血糖和胰岛素时间点后。较低的葡萄糖利用率和较高的 NEFA 水平与 CAC 体积相关(r = -0.42,P < 0.0001 和 r = 0.41,P < 0.0001),并预测 CAC 的存在(比值比 [OR] = 0.45,95%CI = 0.22-0.93,P = 0.03;OR = 2.4,95%CI = 1.08-5.32,P = 0.032,分别)。胰岛素抵抗与 GHb 或连续血糖监测参数不相关。
与非糖尿病受试者相比,1 型糖尿病患者存在胰岛素抵抗,且抵抗程度与当前血糖控制无关。胰岛素抵抗预测冠状动脉钙化的程度,并可能导致 1 型糖尿病患者以及无糖尿病患者的心血管疾病风险增加。