Heart Research Center of Chonnam National University Hospital, Cardiovascular Research Institute of Chonnam National University, Gwangju, Korea.
Korean Circ J. 2010 Oct;40(10):491-8. doi: 10.4070/kcj.2010.40.10.491. Epub 2010 Oct 31.
An elevated concentration of lipoprotein(a) {Lp(a)} is associated with an increased prevalence and increased severity of coronary artery disease. However, the relationship between Lp(a) levels and outcomes after acute myocardial infarction (AMI) is unclear.
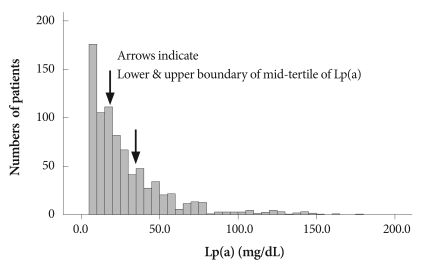
Between October 2005 and June 2007, we measured serum Lp(a) levels in 832 consecutive AMI patients (age, 62.8±12.4 years, 600 men) on admission. They were divided into tertiles according to their serum Lp(a) levels {Tertile 1 (n=276), Lp(a)<13.8 mg/dL; Tertile 2 (n=279), Lp(a)=13.8-30.6 mg/dL; Tertile 3 (n=277), Lp(a)>30.6 mg/dL}.
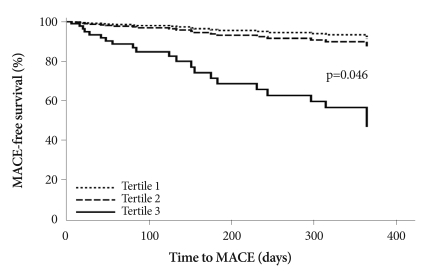
There were no differences in baseline clinical characteristics among Tertiles 1, 2, and 3, except for proportions of Killip class III-IV patients (5.8% vs. 10.0% vs. 18.8%, respectively, p<0.001). There were significant differences in left ventricular ejection fractions (57.3±11.4% vs. 55.9±12.3% vs. 53.1±13.1%, p<0.001). Among the laboratory findings, there were significant differences in total cholesterol (173.3±37.2 vs. 183.5±38.9 vs. 185.3±43.8 mg/dL, p=0.001), low density lipoprotein-cholesterol (111.3±34.3 vs. 122.9±34.7 vs. 123.3±39.4 mg/dL, p<0.001), apolipoprotein B (92.8±25.4 vs. 100.8±26.0 vs. 101.9±28.8 mg/dL, p<0.001), and amino-terminal pro-brain natriuretic peptide levels (1805.2±4343.3 vs. 2607.9±5216.3 vs. 3981.5±7689.7 pg/mL, p<0.001). After adjusting for multiple variables in the high Killip class (III-IV) subgroup, the risk estimate for major adverse cardiovascular events (MACE) at 1-year follow-up was significantly higher in Tertile 3 than in Tertiles 1 or 2 (hazard ratio 6.723, 95% confidence interval 1.037-43.593, p=0.046).
In patients in high Killip classes, high serum levels of Lp(a) were significantly associated with long-term adverse outcomes after AMI.
脂蛋白(a) [Lp(a)]浓度升高与冠状动脉疾病的患病率增加和严重程度增加有关。然而,Lp(a)水平与急性心肌梗死 (AMI) 后的结局之间的关系尚不清楚。
在 2005 年 10 月至 2007 年 6 月期间,我们在 832 例连续的 AMI 患者(年龄 62.8±12.4 岁,600 名男性)入院时测量了血清 Lp(a)水平。他们根据血清 Lp(a)水平分为三分之一{第 1 三分之一(n=276),Lp(a)<13.8mg/dL;第 2 三分之一(n=279),Lp(a)=13.8-30.6mg/dL;第 3 三分之一(n=277),Lp(a)>30.6mg/dL}。
除了 Killip 分级 III-IV 的比例(分别为 5.8%、10.0%和 18.8%,p<0.001)外,Tertile 1、2 和 3 的基线临床特征无差异。左心室射血分数存在显著差异(分别为 57.3±11.4%、55.9±12.3%和 53.1±13.1%,p<0.001)。在实验室检查结果中,总胆固醇(173.3±37.2、183.5±38.9 和 185.3±43.8mg/dL,p=0.001)、低密度脂蛋白胆固醇(111.3±34.3、122.9±34.7 和 123.3±39.4mg/dL,p<0.001)、载脂蛋白 B(92.8±25.4、100.8±26.0 和 101.9±28.8mg/dL,p<0.001)和氨基末端脑钠肽前体水平(1805.2±4343.3、2607.9±5216.3 和 3981.5±7689.7pg/mL,p<0.001)存在显著差异。在高 Killip 分级(III-IV)亚组中调整多个变量后,第 3 三分之一的主要不良心血管事件(MACE)风险估计在 1 年随访时明显高于第 1 或第 2 三分之一(危险比 6.723,95%置信区间 1.037-43.593,p=0.046)。
在高 Killip 分级的患者中,血清 Lp(a)水平升高与 AMI 后长期不良结局显著相关。