Institute of Oncology, Davidoff Center, Rabin Medical Center, Petah Tikva, Israel.
J Natl Cancer Inst. 2010 Dec 15;102(24):1845-54. doi: 10.1093/jnci/djq409. Epub 2010 Nov 23.
Dose-dense chemotherapy has become a mainstay regimen in the adjuvant setting for women with high-risk breast cancer. We performed a systematic review and meta-analysis of the existing data from randomized controlled trials regarding the efficacy and toxicity of the dose-dense chemotherapy approach in nonmetastatic breast cancer.
Randomized controlled trials that compared a dose-dense chemotherapy protocol with a standard chemotherapy schedule in the neoadjuvant or adjuvant setting in adult women older than 18 years with breast cancer were identified by searching The Cochrane Cancer Network register of trials, The Cochrane Library, and LILACS and MEDLINE databases (from January 1966 to January 2010). Hazard ratios (HRs) of death and recurrence and relative risks of adverse events were estimated and pooled. All statistical tests were two-sided.
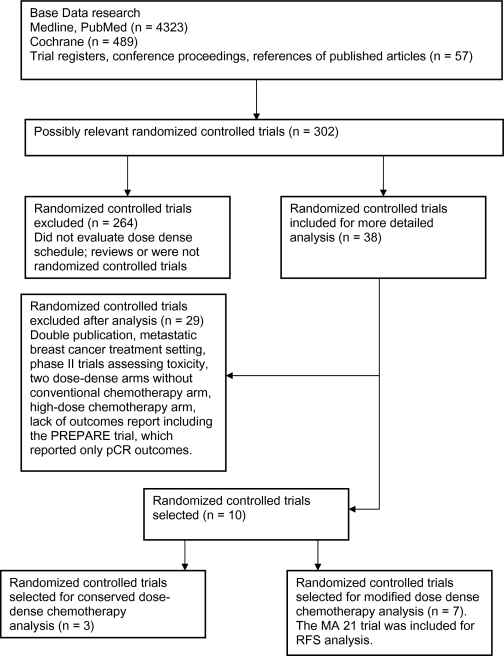
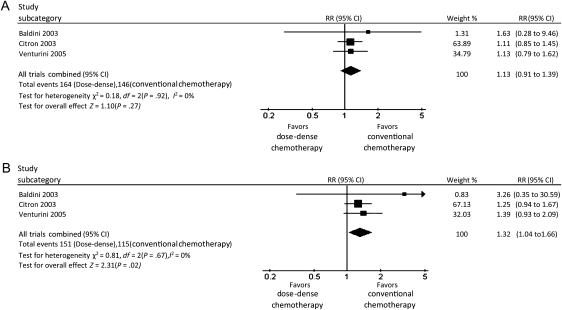
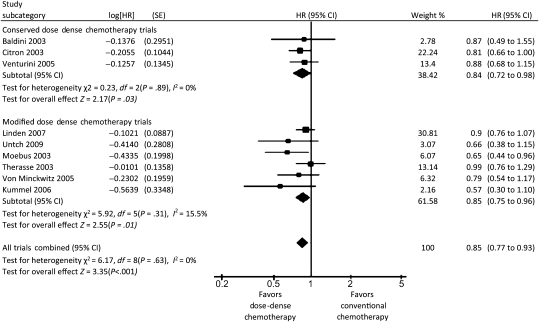
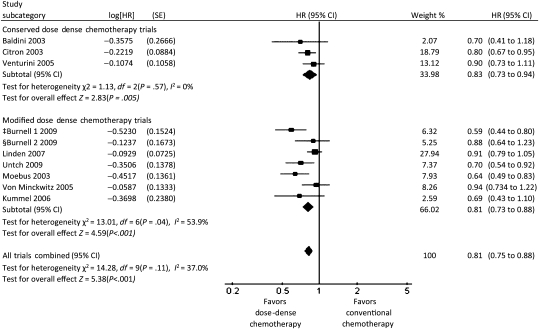
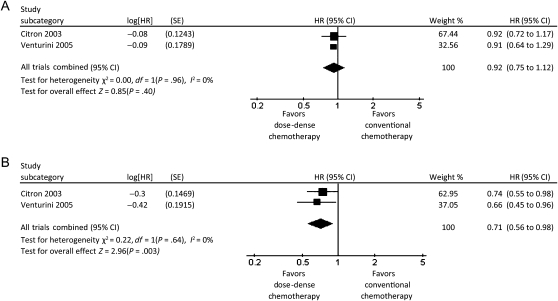
Ten trials met the inclusion criteria and were classified into two categories based on trial methodology. Three trials enrolling 3337 patients compared dose-dense chemotherapy with a conventional chemotherapy schedule (similar agents). Patients who received dose-dense chemotherapy had better overall survival (HR of death = 0.84, 95% confidence interval [CI] = 0.72 to 0.98, P = .03) and better disease-free survival (HR of recurrence or death = 0.83, 95% CI = 0.73 to 0.94, P = .005) than those on the conventional schedule. No benefit was observed in patients with hormone receptor-positive tumors. Seven trials enrolling 8652 patients compared dose-dense chemotherapy with regimens that use standard intervals but with different agents and/or dosages in the treatment arms. Similar results were obtained for these trials with respect to overall survival (HR of death = 0.85, 95% CI = 0.75 to 0.96, P = .01) and disease-free survival (HR of recurrence or death = 0.81, 95% CI = 0.73 to 0.88, P < .001). The rate of nonhematological adverse events was higher in the dose-dense chemotherapy arms than in the conventional chemotherapy arms.
Dose-dense chemotherapy results in better overall and disease-free survival, particularly in women with hormone receptor-negative breast cancer. However, additional data from randomized controlled trials are needed before dose-dense chemotherapy can be considered as the standard of care.
密集化疗已成为高危乳腺癌辅助治疗的主要方案。我们对现有的随机对照试验数据进行了系统回顾和荟萃分析,以评估非转移性乳腺癌中密集化疗方案的疗效和毒性。
通过检索 Cochrane 癌症网络试验注册库、Cochrane 图书馆、LILACS 和 MEDLINE 数据库(1966 年 1 月至 2010 年 1 月),确定了比较 18 岁以上成年女性新辅助或辅助治疗中密集化疗方案与标准化疗方案的随机对照试验。死亡和复发的风险比(HR)和不良事件的相对风险进行了估计和汇总。所有统计检验均为双侧检验。
10 项试验符合纳入标准,并根据试验方法分为两类。3 项试验共纳入 3337 例患者,比较了密集化疗与常规化疗方案(相似药物)。接受密集化疗的患者总生存(死亡 HR = 0.84,95%可信区间 [CI] = 0.72 至 0.98,P =.03)和无病生存(复发或死亡 HR = 0.83,95%CI = 0.73 至 0.94,P =.005)均优于常规方案组。激素受体阳性肿瘤患者无获益。7 项试验共纳入 8652 例患者,比较了密集化疗与采用标准间隔但治疗臂中药物和/或剂量不同的方案。这些试验在总生存(死亡 HR = 0.85,95%CI = 0.75 至 0.96,P =.01)和无病生存(复发或死亡 HR = 0.81,95%CI = 0.73 至 0.88,P <.001)方面也得到了类似的结果。密集化疗组的非血液学不良事件发生率高于常规化疗组。
密集化疗可改善总生存和无病生存,尤其适用于激素受体阴性乳腺癌患者。然而,在密集化疗可被视为标准治疗之前,还需要更多来自随机对照试验的数据。